Traditionally, anesthesia professionals used formulas and estimations that were inadequate to allow for an individualized choice of Double-Lumen-Endotracheal/Endobronchial Tube (DLT) size for a given patient. Measuring mainstem bronchial diameters on CT scan can optimize DLT placement. Therefore, it would add value to also have the endobronchial outer diameter clearly indicated on all DLT packaging.
Letter to the Editor
Over two decades ago several publications warned anesthesia professionals that traditional formulas and estimations are inadequate to allow for an individualized and appropriate choice of Double-Lumen-Endotracheal/Endobronchial Tube (DLT) size for a given patient.1,2
In a letter to the editor, Dr. Slinger made the important observation that “when we cannot reliably predict a clinically important variable, then we need to measure it.”3 Furthermore, the letter states that “Tubes should be clearly labeled with their maximum tracheal and bronchial diameters so that we can choose the correct tube.”3
We queried our Cardiothoracic Anesthesiology staff and found that the majority use computed tomographic (CT) chest scan images to assist in choosing an individualized and appropriate DLT. This approach agrees with the statement by Hannallah et al. that “CT scan measurement of left bronchial diameter can objectively guide the choice of left DLT size for an individual patient.”2 This would satisfy the first call for action for a more evidence-based patient-centered DLT choice.
The second call for action and current weak link in our system is how to compare the measurements obtained on CT imaging to the measurements seen on DLT packaging. One can obtain the endotracheal but not the endobronchial size from current packaging and package insert (Figure 1). To solve this dilemma, our staff often refer to size tables from previous publications,1,2 although data from these publications note manufacturer variability in diameter sizes. We are not aware of a standardized process for manufacturing or labeling DLTs. For example, a specific sized DLT from one manufacturer may have a different outer endobronchial diameter compared to the same sized DLT from another manufacturer. Figure 2 demonstrates a simple technique for determining endobronchial tube diameter. We measured the Shiley (Covidien, Mansfield, MA) DLT with precision calipers and found that the outer endobronchial measurements differed from other manufacturers’ based on previous publications provided by Mallinckrodt (Table 1).1,2
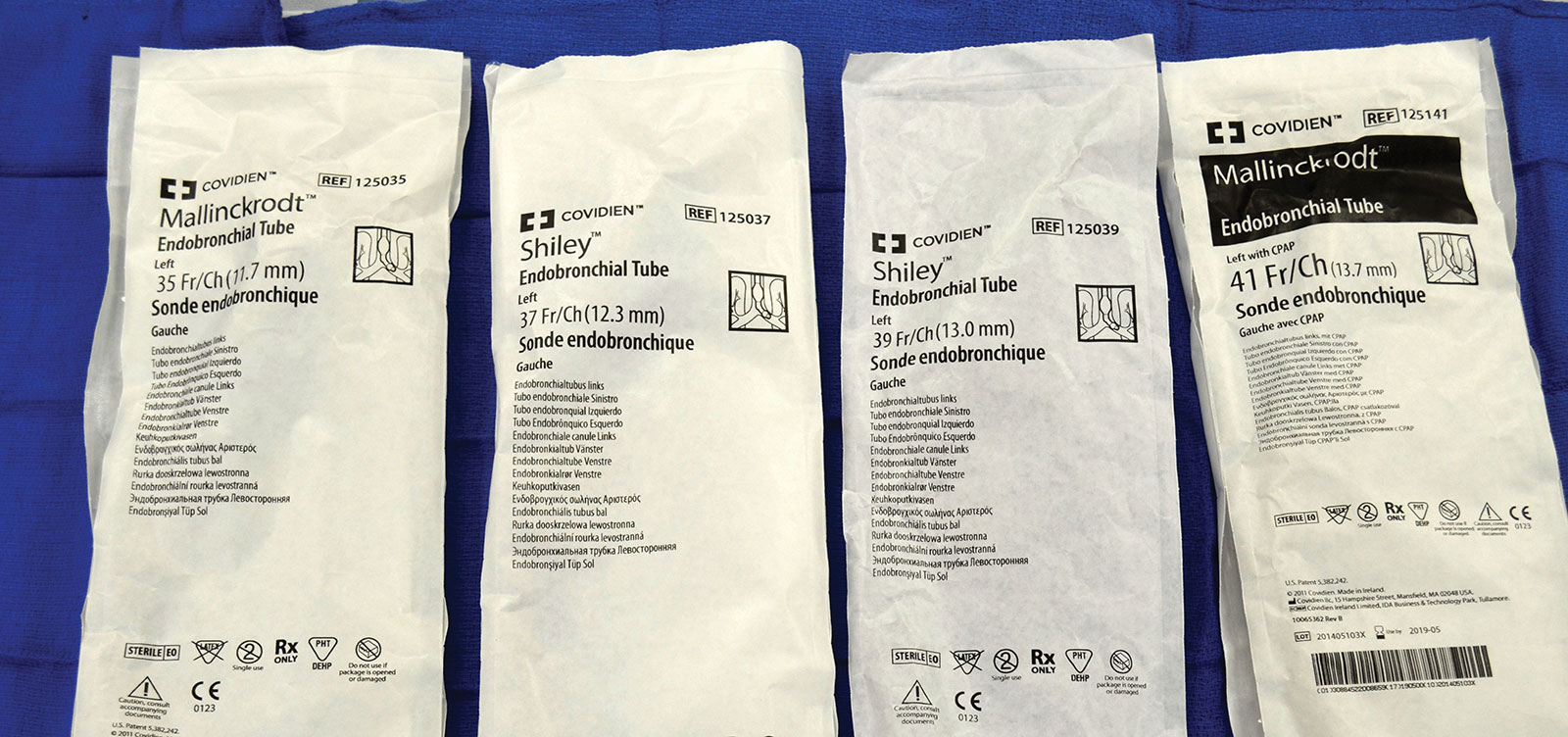
Figure 1: Examples of endobronchial diameters not indicated on Shiley or Mallinckrodt (Covidien, Mansfield, MA) DLT packaging.
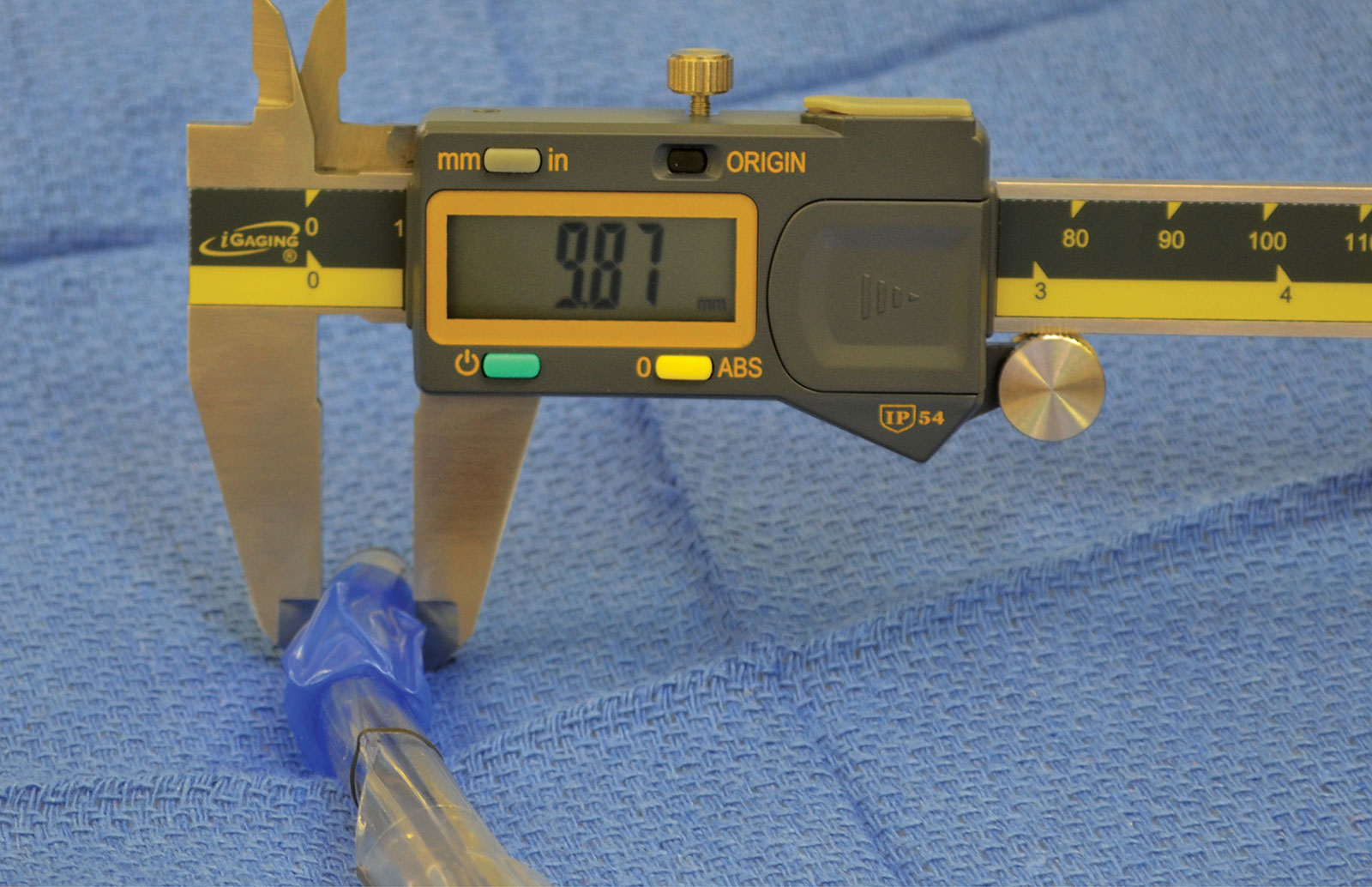
Figure 2: Example of a Shiley 37 Fr Left DLT endobronchial measurement (in mm, this important endo-bronchial diameter is not indicated on the packaging, see Fig. 1).
Table 1: Outer tube diameter measurements of available DLTs (Shiley and Mallinckrodt) from our facility
| DLT Size (avail. for measurement) |
Endotracheal Diameter (mm) | Endobronchial Diameter (mm) |
| 35 Fr Left (3) | 11.92 12.29 11.84 |
9.56 9.48 9.59 |
| Average | 12.02 | 9.54 |
| 37 Fr Left (4) | 12.31 12.80 12.52 12.87 |
9.87 9.90 9.93 9.97 |
| Average | 12.63 | 9.92 |
| 39 Fr Left (4) | 13.26 13.04 13.21 13.37 |
10.30 10.16 10.08 10.25 |
| Average | 13.22 | 10.20 |
| 41 Fr Left (2) | 13.45 13.73 |
10.87 10.74 |
| Average | 13.59 | 10.81 |
We are already one step closer to minimizing iatrogenic bronchial DLT injury to our patients by measuring main bronchial diameters on CT as suggested by Hannallah et al.2 To now find the optimal DLT, we need the second piece of information. We believe the outer endobronchial diameter should also be clearly indicated on the package, and not merely the endotracheal diameter. This would then satisfy both requirements for an optimal patient-DLT-match. This would seem to be an easy improvement process, as it only requires the manufacturer to add the product specification “bronchial diameter” to the package for clinicians’ perusal.
Dr. McDaniel is a CA3 anesthesiology resident in the Department of Anesthesiology, University of Florida College of Medicine.
Dr. Hegland is courtesy assistant professor of Anesthesiology and VA site director in the Department of Anesthesiology, University of Florida College of Medicine.
Dr. Nikolaus Gravenstein is professor of Anesthesiology, Neurosurgery & Periodontology in the Department of Anesthesiology, University of Florida College of Medicine.
Dr. Goldstein is courtesy assistant professor of Anesthesiology and director of Clinical Affairs & Medical Informatics, and co-director of the TAVR Program in the Department of Anesthesiology, University of Florida College of Medicine.
The authors have no conflicts of interest pertaining to this article.
Editor’s Note: We have reached out to a variety of companies to address this issue and an article will be forthcoming in a future APSF Newsletter issue. Several vendors who manufacture double lumen endotracheal tubes have been contacted by APSF and are investigating the possibility of adding bronchial lumen size labeling to the product packaging.
References
- Brodsky J, Macario A, Mark JB. Tracheal diameter predicts double-lumen tube size: a method for selecting left double-lumen tubes. Anesth Analg. 1996;82:861–864.
- Hannallah M, Benumof JL, Silverman PM, et al. Evaluation of an approach to choosing a left double-lumen tube size based on chest computed tomographic scan measurement of left mainstem bronchial diameter. J Cardiothorac Vasc Anesth. 1997;11:168–171.
- Slinger P. Choosing the appropriate double-lumen tube: a glimmer of science comes to a dark art. J Cardiothorac Vasc Anesth. 1995;9:117–118.
