To the Editor
The following are excerpts from the introduction to the series on patient safety that appeared in the New England Journal of Medicine.1
- The central message of the recently released Institute of Medicine (IOM) report, “To Err Is Human” was that errors are caused more by faulty systems than individual carelessness.
- The IOM report made 4 major points: the problem of accidental injury is serious, the cause is not careless people but faulty systems, we need to redesign our systems, and patient safety must become a national priority.
- The concept that errors result largely from the failures of systems, not from individual carelessness or inadequacy, is fundamental to the new effort to address safety and runs counter to the traditional focus of medical training on individual performance. However, the concept is based on a wealth of studies in cognitive psychology and human-factors engineering, as well as substantial experience in other industries, showing that achieving safety requires more than a reliance on individual carefulness.
- Changes based on this concept were first introduced into health care in the 1980s by anesthesiologists. Mortality related to anesthesia was dramatically reduced by the use of critical-incident analysis, standardization, and checklists, as well as changes in training and supervision and the nearly universal implementation of new monitoring techniques.
- Making changes is compounded by the tendency to assign blame for errors, fear of lawsuits, and a focus on individual performance. Not surprisingly, the pressure to improve patient safety has met with some resistance. One concern is that the focus on the system will reduce individual accountability or that the emphasis on safety will divert attention from other aspects of the quality of care.
- An important barrier to improving patient safety is the confusion and misunderstanding about what the new systems approach entails and how to reconcile it with the need for individual and collective accountability.
These observations were generated as a result of the IOM’s report titled “To Err is Human: Building a Safer Health System.”2 Recently, Leape and Berwick published a follow-up to the IOM report titled “Five Years After To Err Is Human. What Have We Learned?”3 They note that improvements are still possible:
“Five years ago, the Institute of Medicine (IOM) called for a national effort to make health care safe. Although progress since then has been slow, the IOM report truly “changed the conversation” to a focus on changing systems, stimulated a broad array of stakeholders to engage in patient safety, and motivated hospitals to adopt new safe practices. The pace of change is likely to accelerate, particularly in implementation of electronic health records, diffusion of safe practices team training, and full disclosure to patients following injury.”
In keeping with the belief that errors result largely from the failures of systems, I would like to point out 3 potentially dangerous anesthesia-related system problems whose easy correction would help prevent adverse outcomes:
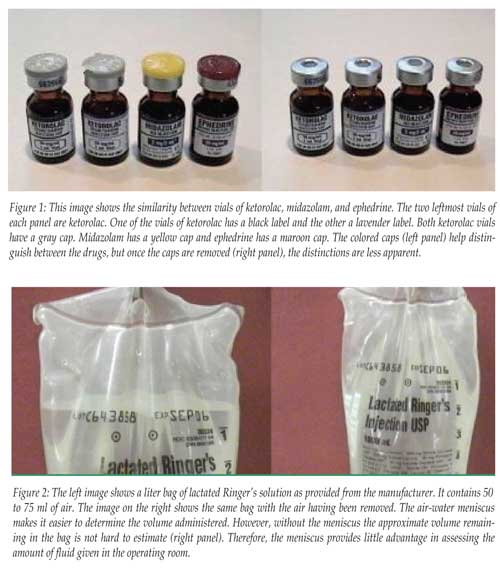
- The first is the similarity in appearance and labeling of drugs (Figure 1). This image shows 4 vials that I recently pulled from a drug tray provided to our anesthesia service by the hospital pharmacy. I was struck by the similarity of the vials as I looked for a vial of ephedrine. The manufacturer apparently attempts to avoid drug swaps by color coding the vial tops (Figure 1, left panel). However, once the caps are removed the vials appear strikingly similar (Figure 1, right panel), making a drug swap extremely easy. A better solution would be to color code the labels and/or change the shape of the vials. For example, potentially dangerous vasoactive drugs could have red labels or be put in square instead of round bottles.
- The second is the preparation of intravenous fluid bags with air in them. The intravenous fluid bags that are used at my institution contain 50 to 75 ml of air. The problem arises during operations where a lot is happening quickly. When IV bags run dry, a few milliliters of air usually enters the IV tubing, making it necessary to purge the air from the tubing. In an operation where events are changing rapidly (e.g., trauma operations), this is a time-consuming distraction. More important is the problem encountered when IV bags are pressurized to give the fluid rapidly for volume resuscitation. Under these conditions the 50 to 75 ml of air can enter the venous circulation and cause hemodynamic compromise. A worst case scenario would be air entering the CNS or coronary arteries in a patient with an unknown septal defect. Eliminating the air from the bag when spiking it with the IV tubing can minimize air embolism. However, this is time-consuming, and when rapid volume resuscitation is required, purging the air from the bag is inconvenient and often forgotten. This may precisely when venous air embolism is most likely to happen. A better resolution is to manufacture the bags without air in them. Figure 2 shows a liter bag of IV fluid with air (left) and without air (right). The air-water meniscus does make it easier to determine the volume administered, but even without the meniscus the approximate volume remaining in the bag is not hard to estimate (Figure 2, right panel). Thus, the amount of fluid given is not hard to determine, and the advantage that the meniscus provides in operating room fluid management is minimal.
- The third system alteration to improve patient safety concerns the daily practice of diluting potentially dangerous vasoactive drugs for the treatment of hypotension. This time-consuming and wasteful ritual occurs daily in all operating rooms. The worst case scenario involves a drug swap where epinephrine is accidentally diluted in the belief that it is ephedrine. Some spinal trays contain epinephrine and ephedrine, making this a distinct possibility. Other swaps of phenylephrine for ephedrine or epinephrine are also possible. A more common error is that which occurs with calculating and making the proper dilution. Also, how much time is wasted daily making these calculations and dilutions? Hospitals no longer ask their staff to dilute KCl because of dilution errors that have caused deaths. It would be an easy system change for drug manufacturers to produce color-coded, 10-ml syringes pre-loaded with ephedrine (5 mg/ml) or phenylephrine (100 mcg/ml). These prepackaged syringes would have a longer shelf-life than those drugs that are manually diluted, and prepackaged syringes would eliminate the enormous waste owing to discarding the manually diluted drugs at the end of each day.
I do not believe that drug swaps will ever be totally prevented, nor am I suggesting that anesthesiologists not be vigilant. It is always good practice to check a vial 3 times: once before opening it, a second time when removing the agent, and a third time before discarding the vial. I do believe, however, that the system changes I propose here will eliminate some of the otherwise inevitable drug swaps.
Donald H. Lambert, PhD, MD
Concord, VT
References
- Leape L, Epstein AM, Hamel MB. A series on patient safety. N Engl J Med 2002; 347 1272-4.
- Kohn, LT, Corrigan, JM, and Donaldson, MS, editors; Committee on Quality of Health Care in America, Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press, 2000.
- Leape LL, Berwick DM. Five years after To Err Is Human: what have we learned? JAMA 2005;293:2384-90.
