Placing a label on an otherwise unmarked syringe containing a drug intended for intravenous use would seem an uncontroversial contribution to patient safety. Yet 20 years after the original specification was published, we still await universal acceptance of the idea.
The Problem
The need for such a marker has existed since those early days in anesthesia when intravenous barbiturates first challenged inhaled drugs at Pearl Harbor, and when Cecil Gray established the pivotal role of curare in general anesthesia. The speed of response to an intravenous (IV) injection may not allow time to manage the consequences of an error, and use of the IV route in general anesthesia has become more widespread. Many of us have devised systems for labeling our drugs. But now, the single anesthesiologist or anesthetist, once independently responsible for patient well-being during surgical assault, is being integrated into a surgical team, where responsibility for most aspects of a patient’s care is shared; others now expect insight into the gasman’s codes. So our once simple labeling system, designed as a rapid recognition code for the anesthesiologist or anesthetist, now has to evolve into a nationally agreed code for the precise recognition of pre-prepared injectable drugs for use by other surgical team members.
How it Started
In the mid 1950s the University of Stellenbosch started planning a new medical school campus in Cape Town, South Africa, that would integrate medical, dental, and nursing schools with a major general hospital. All of this came into being in the early 1970s as the largest “school under one roof” in the Southern hemisphere, known as the Tygerberg Hospital. Design ideas were sought throughout Britain, Europe, and the United States, and major equipment sources were expected to come from Britain. However, 6,000-mile supply lines and misunderstandings of local circumstances meant that needs were often best met by local design and manufacture. Against this background, the incidental production of a syringe labeling system for a large anesthesia service was a minor undertaking, supported by the local Anesthesia Society. After testing designs in the mid 1970s Avery printed the original design and supplied international color definitions in the national specification. Rolls, each with 100 individual names on the code color, were mounted alongside each other on a dowel comprising a multiple dispenser. Some colors were chosen to reflect the class characteristics: “danger” red for muscle relaxants; blue to signify the cyanosis of opiate-induced respiratory depression; green for atropine-like drugs used in a syringe size smaller than (red) relaxants. There were few specific antidotes to the IV drugs used in anesthesia, but these were considered important enough to have some link to the color code of the agonist. This was done by using diagonal white stripes and color stripes in the color bar of the agonist. Thus nalorphine, atropine, and flumazenil share the color of opiates, relaxants, or benzodiazepines, respectively. With mixtures some interesting stripe patterns emerged, such as red/green/white alternating for the usual standard relaxant reversal of neostigmine and anticholinergic.
Visiting anesthesiologists to the Tygerberg Hospital took labels home to the United Kingdom, many European countries, Canada, and the United States, thus leading to the development of several informal versions. Dr. Rendell Baker was one of the first to introduce these ideas to the United States.
The original specifications were published in 1985 by the South African Bureau of Standards as SABS 0207-1985, and placed in the catalog of the International Standards Organization, of which the SABS is a member. Currently this standard is published by the Standards South Africa division of the SABS as SANS 10207 (www.stansa.co.za). A second revision is now under preparation to appear on this 20th anniversary of the original.
A Need for Change
After 20 years a revision is necessary, if only to incorporate the changes brought by new technology. There were few applications for computers in a 1970s OR, but today, a syringe label can provide the interface between anesthesia machine and a computer that can “autopilot” a general anesthetic while recording the data. A revision also provides a chance to revisit some of the basic aims that shaped the first standard, which sometimes may have been misunderstood. There were drug representatives who believed the labels would replace the identifying “house colors” of their products. (Today, some makers wishing to support the color code concept, pack drugs of a similar class in boxes of the specified color. This is even more dangerous since drugs such as ephedrine and epinephrine can be mixed up in the same drawer of a drug cart stocked by a junior aid). The main goal was to reduce the danger of the wrong IV injection during the process of anesthesia. A design was proposed for a series of labels easily identifiable by color and print. These were to be applied to any syringe containing any drug, intended for IV use, after it had been transferred from its original pack into an anonymous syringe. Implied in the standard is observance of the safe practice that only the ultimate user of an IV drug should prepare the injection and affix the label. For optimum safety, it is essential to use one standard design as variations may lead to confusion.
Originally the focus of the 1985 standard was on anesthesia practice; however, this need now extends to cover PACU or postoperative ICU care. Recently, JCAHO regulations have addressed a wider range of drugs:
“A new requirement for all types of accredited organizations that provide surgical or other invasive services specifies that all medications, medication containers, and other solutions used in peri-operative settings be labeled.”
This innovation, that includes syringes with other medication containers, seems eminently reasonable so long as one notes the following items:
First, a single unlabeled syringe is an anathema; unidentified content is presumed dangerous and to be discarded. Creative solutions will be found to cover simple routine clinical procedures such as the “flu shot.” For example, “Provided that the syringe never leaves the hand of the user from the time of its loading from a manufacturer’s container until its discharge, no label need be applied.” Second, the simplest label must now include four data fields: drug name, drug mass per unit volume, date and time of preparation, and dispenser’s identity. The standard label now used in most OR’s has space for the extra details. Third, these changes are brought about by the challenge to the prime status of the syringe as drug delivery container by the larger medication containers, which deliver more drug over a longer period at less cost in material and supervision. As our “drugs for use in anesthesia” is revised to become “drugs for use in anesthesia and intensive care,” so must our designs include new large containers labels with extra data fields relevant to the longer stay within an intensive care system. For this use present syringe labels are too small. Will there be 24-48 hour labels, 7 day specials, or Medicare monthly concessions?
We approach an era when general anesthesia, once provided by the skilled hand, operating a gas dispenser to meter oxygen flows and narcotic vapors, is to be replaced by a ventilator controlled by a dedicated computer that drives a series of gas and infusion meters. As a stranger among these binary controls, may there still be a handheld syringe? Will some experience nostalgia for the days of one provider responsible for the full care of one patient at a time?
On Basic Design
The widespread acceptance of the color coded label system almost certainly depends on easy recognition of a pattern that combines 3 simple elements: the syringe size, label color, and printing. Most times a person will use several drugs, from different classes, as identified by the color code, and each in a syringe large enough for the dose. Often, it is possible to pick out a drug from across the room by the syringe size and color, at a distance where printing would be illegible. Print confirms an initial selection based on syringe size and color pattern. Critics of the system object that color blindness must make the system unreliable. Years of full acceptance and recently a well designed study1 have shown this to be untrue.
Why aren’t our traffic signals red, amber, and blue to suit our many red/green blind users? In fact, this use of color has proven valuable with the small label size imposed by the size of a 2-3 ml syringe: a whole colored label stuck on a rounded surface is easier to interpret than the print.
Enlarging the Code
Should the color code be enlarged to include all drugs used in intensive care as some enthusiasts suggest? I believe that the acceptance of the present system has depended in large part on its simplicity; from the start it was never intended to include all classes in the pharmacopoeia. It would be difficult to find more than about 15 distinct colors and for most users to memorize all 15 (when they daily rely on only 5 or 6 classes in most patients). There are 1 or 2 colors still “available”. That should be enough. Meanwhile a white label can be used for all other drugs while the role for color coding remains safe with anesthesia.
In passing, one notes that there are other accepted color codes for volatile anesthetics and for compressed gases that do not interact with the label code.
Code could be extended by extra markings on a syringe. Better than color coded syringe caps would be a form of coding, color or print, on the thumb plate of the plunger. One could suggest a use to indicate the refrigerated shelf life of pre-filled syringes from a central pharmacy. Stacked syringes are then sorted by end colors.
The Role for Barcodes
Two questions still await a good answer; what are you going to code, and who will be reading it? With the inclusion of critical care in our label code, there may now be a role for such a vehicle for rapid, accurate patient data transfer. JCAHO, in the document quoted above, places special emphasis on full, accurate data transfer at every patient “hand off” (transfer) between caregivers. The syringe label even has limited space for small barcodes, although the value could be in routine anesthesia may be difficult to see.
Reading barcode requires a computerized scanner. Ultimately this can take the form of a peripheral syringe reader-driver that also detect drug and volume in the syringe by reading code, and, by, following plunger head movement, record dose and time.
Printed Labels
Do people realize that buying into a system of pre-printed labels can lead to a problem? One assumes that members of a department first agreed to their label list of standard drug names and doses. This means that an unscheduled format must be signaled using a (non-color code) white label. Real danger may arise when drug indicates an “almost the same” drug, as when the name remains unchanged but concentration is only changed on the label. If a standard label is used, flag it. Otherwise a user, seeing the familiar color and drug name, might miss the small following figure.
(Was it thiopentone 2.5% or 5%? Did you dilute the sufentanil?).
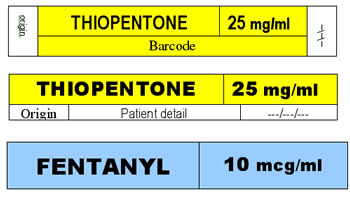
Until final decisions are made, new label designs might appear as shown.
The practical value of color codes on syringes lies ultimately in ease of use. With a color printer sheets of labels can be printed and kept in a loose-leaf cover. Simpler, but more costly, is to buy rolls of 100 preprinted labels and mount a series on a dowel as dispenser. More elegant and versatile might be an adaptation of a dedicated label printer programmed to produce any selected drug, name, color, and dose, with today’s date and preparer. It might even barcode patient name, age, sex, weight. But for millions this last will remain a dream wherever basic drugs, syringes, even oxygen, are still on their wish list.
Patrick Foster is a Professor Emeritus in the Department of Anesthesia, Penn State University, Milton S. Hershey Medical Center, Hershey, PA.
Reference
- Cumberland P, Rahi JS, Peckham CS. Impact of congenital colour vision deficiency on education and unintentional injuries: findings from the 1958 British birth cohort. BMJ 2004;329:1074-5.
