Episode #312 Hantavirus Readiness For Anesthesia Teams
June 24, 2026
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is an APSF Newsletter article published online May 19, 2026. It is “Hantavirus Awareness for Anesthesia and Critical Care Professionals” by Jonathan E. Charnin, MD FASA; Brendan T. Wanta, MD; Randy W. Loftus, MD.
Here are the quick facts about Hantavirus from the Figure in the article:
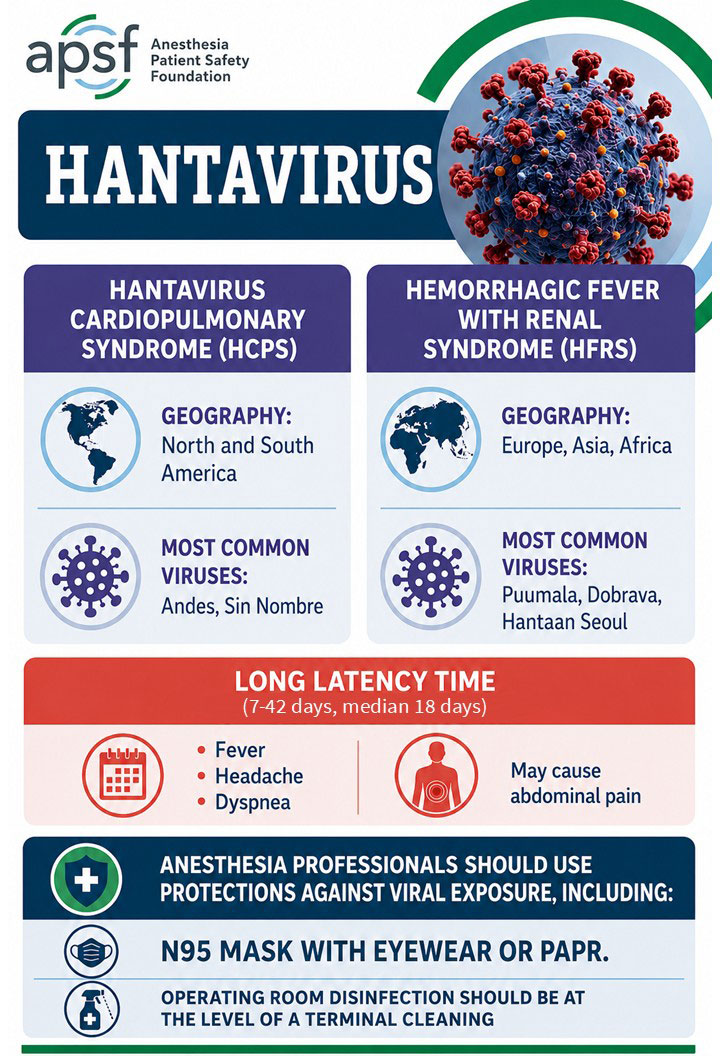
Figure Legend: Hantavirus Facts at a Glance. Microsoft Copilot was used to generate a draft of this infographic, which was later modified by Arney Abcejo, MD.
Check out these resources for a demonstration of personal protective strategies:
- https://www.youtube.com/watch?v=C2pT1jg5QUs
- https://www.apsf.org/news-updates/optimizing-infection-control-and-or-management-during-the-covid-pandemic/
Next, we review the “Response to Hantavirus Awareness for Anesthesia and Critical Care Professionals” by Brent Lee, MD, MPH, FASA. This article was published online May 21, 2026.
Here are the citations to the articles that we talked about on the show today.
Citations:
- Maes P, Tischler N. Statement from the International Hantavirus Society and members of the international hantavirus research and clinical community regarding Andes virus transmission and the current outbreak investigation. International Hantavirus Society. Published May 12, 2026. Accessed May 13, 2026. Available at: https://zenodo.org/records/20134326
- Martinez VP, Di Paola N, Alonso DO, et al. “Super-Spreaders” and Person-to-Person Transmission of Andes Virus in Argentina. N Engl J Med. 2020;383(23):2230–2241. PMID: 33264545
- Ferrés M, Martínez-Valdebenito C, Henriquez C, et al. Viral shedding and viraemia of Andes virus during acute hantavirus infection: a prospective study. Lancet Infect Dis. 2024;24(7):775-782. Erratum in: Lancet Infect Dis. 2024;24(7):e419. PMID: 38582089
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2026, The Anesthesia Patient Safety Foundation
Opening Clip: [Brent Lee] “Unfortunately, whether it’s this strain of the hantavirus or the rapidly spreading Bundibugyo Ebola virus, I do believe that another major emerging infectious disease outbreak or worldwide pandemic is not a matter of if, but when. I believe that the knowledge, skills, and training that we as anesthesia clinicians possess are invaluable in large-scale emergencies, whether they’re pandemics, mass casualty events, natural disasters, or the care of casualties of large-scale combat operations. My hope is that more anesthesia clinicians will become engaged in health security and large-scale emergency preparedness and response in the future.”
Hello and welcome back to the Anesthesia Patient Safety Podcast. I’m your host, Alli Bechtel. Here are some quick Hantavirus facts and information about the recent outbreak. It is a single-stranded RNA zoonotic virus that usually infects small rodents with little impact on the host. On May 6th, the World Health Organization confirmed a Hantavirus infection cluster caused by the Andes virus which is endemic in areas of South America. The Andes virus is the only hantavirus known to be able to spread person-to-person, usually following prolonged and close contact. By the 15th of May, there were 10 cases including 3 deaths. Today, we are discussing everything you need to know about Hantavirus infection to help keep you and your patients safe during anesthesia care, so stay tuned.
Before we dive further into the episode today, we’d like to recognize Fresenius Kabi, a major corporate supporter of APSF. Fresenius Kabihas generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Fresenius Kabi – we wouldn’t be able to do all that we do without you!”
Our featured article is “Hantavirus Awareness for Anesthesia and Critical Care Professionals”
by Charnin and colleagues. This is a APSF Newsletter Article that was published online May 19th, 2026. To follow along with us, head over to APSF.org and click on the Newsletter Heading. The first one down is Newsletter articles. Then, you can scroll down until you get to our featured article, and I will include a link in the show notes as well.
The most common transmission pathway for human Hantavirus infection involves inhalation of aerosolized viral particles while cleaning rodent droppings. Contact with rodent saliva can also lead to infection. Disease latency is variable with an incubation period of 7-42 days. This makes it difficult to identify the original exposure. If we look at Hantavirus around the world, there are the Andes and Sin Nombre viruses that cause Hantavirus Cardiopulmonary Syndrome in the Americas. Haemorrhagic Fever with Renal Syndrome is caused by the Hantaan and Puumala viruses in Europe, Asia, and Africa. The case fatality rate from Hantavirus Cardiopulmonary Syndrome, which is associated with severe respiratory failure, is really high at 10-50%. Haemorrhagic Fever with Renal Syndrome may lead to bleeding and renal failure with a fatality rate of 1-12%. Hantavirus attacks capillary endothelial cells leading to increased capillary permeability and noncardiogenic pulmonary edema in both syndromes. Check out the Figure in the article for a quick review of Hantavirus infections for anesthesia professionals. You can find it in the show notes as well.
Let’s take a closer look at Hantavirus transmission. At this time, the Andes virus is the only one known to spread person-to-person. There was a 2011 outbreak of the Andes virus that involved transmission to close contacts during the febrile illness leading to infection. The close contacts included spouses who shared a bed or healthcare professionals involved in direct patient care. During another Andes virus outbreak in 2018, there was no nosocomial transmission even to healthcare professionals involved in high-risk procedures such as intubation. It is likely that transmission depends on significant exposure to bodily fluids, especially saliva, from an infected person during the prodromal phase of the illness. Keep in mind that there is a long latency phase so confirming person-to-person spread is often difficult. If we look at the most recent outbreak on the cruise ship, it is likely that extended contact or shared living spaces played a role in the person-to-person spread.
Now it’s time to evaluate the clinical features of Hantavirus infection. Patients may develop fever, myalgias, backache, and headache initially. Severe abdominal pain has been reported which presents as an acute abdomen. Patient have been taken to the operating room for appendectomy and then were later diagnosed as having Hantavirus infection. Disease progression may include thrombocytopenia, oliguria, kidney injury, and respiratory failure. Severe respiratory failure is more likely to occur with Hantavirus Cardiopulmonary Syndrome. The highest concentration of viral particles is found in the blood, but may be in other bodily fluids, so there is a risk of nosocomial viral transmission. Testing for Hantavirus is with PCR techniques and in the United States, a clinical PCR test for the Andes virus is under development. Antibody testing may also be used later in the infection. There are moderately effective vaccines for Haemorrhagic Fever with Renal Syndrome available in Korea and China. It is important to report Hantavirus infections to local public health officers and patients with suspected or confirmed infection should be evaluated by infectious disease team and hospital infection control. Treatment for Hantavirus is supportive care and in cases of respiratory failure, ECMO may be considered as a bridge to recovery. Viral therapy has been studied, and treatment with ribavirin alone was not effective. Combination therapy with ribavirin and favipiravir has been shown to work against the virus in-vitro and further research is needed in this area.
Let’s move this discussion into the perioperative space and operating rooms, but I warn you we will be proceeding without recommendations. This is a difficult situation. Often the exposure timing is only determined in retrospect and there is a long latency with this infection. For elective surgery considerations, you may consider delaying elective surgery for patients with a known exposure until after the patient is through the latent period, about 39 days. Patients with acute Hantavirus infection should have elective surgery delayed until return to full health, which may be months later. For emergency surgery for patients with Hantavirus infection, be prepared for bleeding due to thrombocytopenia and coagulation system dysfunction. Following surgery, patients will need to recover in a negative pressure isolation room.
When it comes to infection control, what protective strategies are recommended to prevent nosocomial transmission? Hantaviruses are enveloped and similar in size to the SARS-CoV-2 virus so similar protective strategies should be used. There are some institutions that use the highest level of precaution similar to other haemorrhagic fevers like Ebola and Marburg. Check out the show notes to a video demonstration of the recommended protective strategies.
And here are the recommendations for anesthesia professionals when providing care for patients with known or suspected Hantavirus infection.
- N95 masking or powered-air purifying respiratory use during airway management and any aerosol-generating procedures.
- Eye protection
- Due to the small size of the virus, personal use of nasal povidone iodine in conjunction with masks may be considered.
- A gargle of dilute 1:10 povidone iodine in water may also be used for additional protection.
- Hand hygiene should be used with alcohol-based hand sanitizers
- Designation of clean and dirty areas within the anesthesia workspace.
- After induction of anesthesia, perform a top cleaning of the anesthesia machine and equipment with quaternary ammonium compound and alcohol wipes.
- Needleless ports should be disinfected prior to access
- Between cases, perform a terminal-level operating room cleaning with UV-C irradiation if available using evidence-based approaches.
Next up, we are going to check out the “Response to Hantavirus Awareness for Anesthesia and Critical Care Professionals” by Brent Lee and we happen to have some exclusive content from the author.
[Brent Lee] “ Hi, I’m Brent Lee, and I am the Director of Clinical Excellence and Performance Improvement at North American Partners in Anesthesia and an associated scholar and affiliate at the National Center for Health Security and Resilience at Georgetown University.”
[Bechtel] I asked Brent what got him interested in this topic. Let’s take a listen to what he had to say.
[Brent Lee] “Early in my career, I served as an epidemic intelligence service officer at the CDC. So when the COVID-19 pandemic hit and I was serving as the patient safety officer at NAPA, I saw firsthand the devastation caused by this novel pathogen, not only to the patients we cared for, but also the profound physical and emotional toll it took on our anesthesia clinicians. That experience deepened my interest in health security and specifically the role anesthesia clinicians play in disaster preparedness and response. More recently, I completed a graduate program in biodefense where I happened to write a term paper on hantavirus. So when news emerged about the outbreak on the cruise ship, my immediate thought was our community needs to be as prepared as possible for whatever may be coming down the pike.”
Let’s check out Brent’s response to the editor. He reports that with the recent Hantavirus outbreak aboard the cruise ship, the risk of a pandemic-level threat to the global population is low according to the World Health Organization, but there are reasons to be concerned including high case fatality rate, prolonged and variable incubation period, and no effective vaccine or treatment. There is another important consideration, transmission of the virus. While public health officials have stated that person-to-person transmission is rare and requires prolonged and intimate contact with a symptomatic person, this may not be true according to the currently available evidence.
So, let’s look at the available evidence. The International Hantavirus Society published a statement on May 7th of this year about transmission of the Andes strain of Hantavirus. During the 2018-2019 outbreak in Argentina, there was an index patient with fever and malaise who attended a birthday party for 90 minutes, 5 guests who were seated near this patient became infected. Then, one of these birthday party guests infected 6 other people and later died from the infection. At his wake, his spouse was symptomatic and passed on the infection to 10 people. There were 33 people who became infected during this “super spreader” outbreak with 11 deaths. If we look at the cruise ship outbreak, there are some parallels, since many of the infected patients, the primary known exposures were shared indoor environments in the cruise ship dining rooms and lecture halls.
Another signal from the literature is that patients may not need to be symptomatic to effectively transmit the virus. There is a 2024 publication by Ferres and colleagues, “Viral shedding and viraemia of Andes virus during acute hantavirus infection: a prospective study” that found infective virus in the urine, saliva, and nasopharyngeal secretions before patients developed symptoms. We hope that you will check out the show notes for the citations so that you can check out these studies.
Brent points out that these findings reveal what is possible with hantavirus transmission. Even if this is not how the virus usually behaves, we need to be prepared. This is an area where anesthesia professionals excel. We are trained to be prepared for rare events or for when things don’t go according to plans as evidenced by simulation training for malignant hyperthermia or performing a rapid sequence induction for patients with unknown fasting history.
And speaking of being prepared, it is important to use full airborne and contact precautions when caring for patients with known or suspected Andes hantavirus infection. Other recommendations from the ASA Committee on Occupational Health include the following:
- “If manual or mechanical ventilation is necessary, then place a HEPA filter between the patient’s airway and the distal end of the disposable portion of the breathing circuit.
- Protect the anesthesia gas sampling port with HEPA filtration, or, at a minimum, scavenge the gases exiting the gas analyser and do not allow the gases to return to the room air.
- If temporary disconnection from the breathing circuit is required, keep the HEPA filter attached to the patient’s airway.
- If a portable bag-valve-mask device is used, place the HEPA filter between the device and the patient’s airway to prevent room air contamination.”
Brent reminds us that patients with hantavirus infection may require intensive care with mechanical ventilation, invasive monitoring, ECMO, and careful fluid and electrolyte management. While the public health messaging focus on reassurance and preventing panic, healthcare professionals need to remain prepared and up to date to make safe and informed decisions.
[Bechtel] Before we wrap up for today, we are going to hear from Brent again. I also asked him what he hopes to see going forward. Here’s his response.
[Brent Lee] “ Unfortunately, whether it’s this strain of the hantavirus or the rapidly spreading Bundibugyo Ebola virus, I do believe that another major emerging infectious disease outbreak or worldwide pandemic is not a matter of if, but when. I believe that the knowledge, skills, and training that we as anesthesia clinicians possess are invaluable in large-scale emergencies, whether they’re pandemics, mass casualty events, natural disasters, or the care of casualties of large-scale combat operations. My hope is that more anesthesia clinicians will become engaged in health security and large-scale emergency preparedness and response in the future.”
[Bechtel] Thank you so much to Brent for contributing to the show today.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
Until next time, stay vigilant and stay informed so that no one shall be harmed by anesthesia care.
© 2026, The Anesthesia Patient Safety Foundation
