Hantavirus infection can produce severe disease with a high mortality rate throughout most of the world. Reporting suspected cases to infection control officers is recommended. While person-to-person spread of the disease is uncommon, anesthesia professionals should protect themselves while patients are symptomatic. Treatment for Hantavirus infection is supportive.
| Related Article: Letter to the Editor: Response to Hantavirus Awareness for Anesthesia and Critical Care Professionals |
Hantavirus, a single-stranded RNA virus, is a rodent-borne pathogen that causes serious human disease. Hantavirus has gained notoriety recently due to a cluster of infections with a high mortality rate involving cruise ship passengers in May of 2026.1 In the most recent outbreak, person-to-person viral transmission is suspected. Although human-to-human transmission is rare, here, we outline basic steps that anesthesia professionals can utilize to augment patient and personal protection.
In brief, Hantaviruses are a family of are zoonotic viruses that typically infect small rodents with little impact on their host. Transmission to humans is possible and typically involved aerosolization of rodent feces, but rodent saliva can also be a vector. A typical transmission route involves inhalation of aerosolized viral particles when cleaning rodent droppings. There is variable disease latency, with the incubation period ranging from 7 to 42 days (median 18 days) (Figure).2 The long latency period complicates identification of the point of exposure. In the Americas, the Andes and Sin Nombre viruses primarily causes Hantavirus Cardiopulmonary Syndrome (HCPS). In Europe, Asia, and Africa, the Hantaan and Puumala, among other viruses, cause Hemorrhagic Fever with Renal Syndrome (HFRS). HCPS commonly inflicts patients with severe respiratory failure, while HFRS leads to bleeding symptoms and potential renal failure (Figure). The case fatality of Hantavirus infections with HCPS is approximately 10 to 50 percent, while case fatality from HFRS is lower at 1 to 12 percent.3 Capillary endothelial cells are the primary viral targets for both syndromes, resulting in increased capillary permeability and noncardiogenic pulmonary edema. Hantaviruses are classified with other hemorrhagic fevers, but person-to-person spread is much less common than is seen with other hemorrhagic fevers such as Ebola.
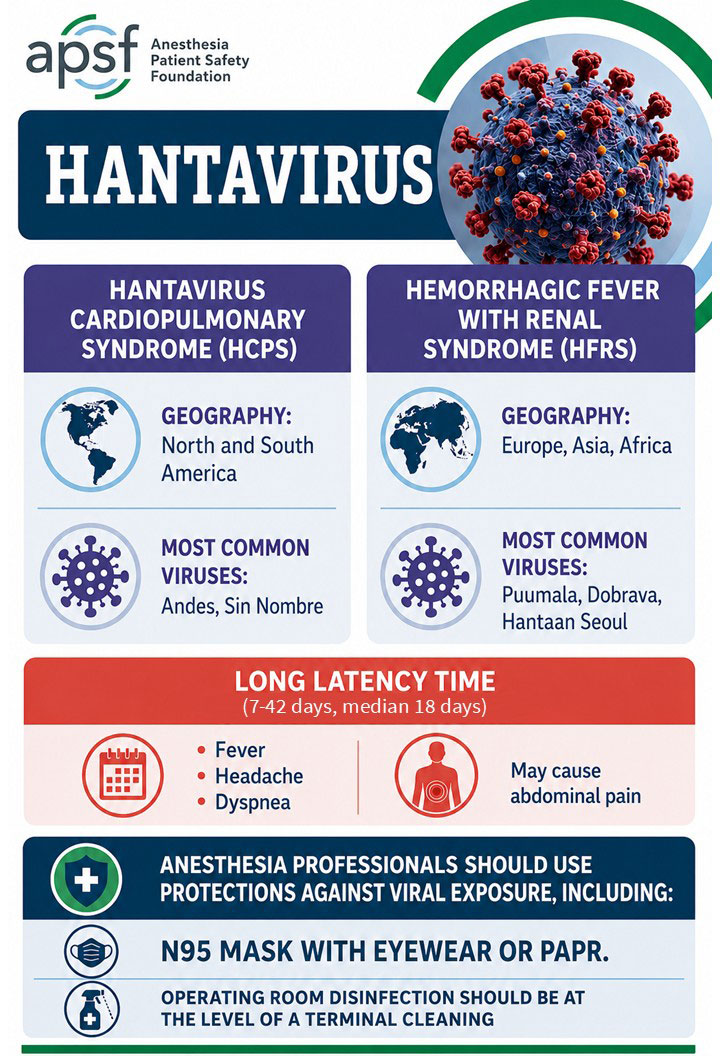
Figure Legend: Hantavirus Facts at a Glance. Microsoft Copilot was used to generate a draft of this infographic, which was later modified by Arney Abcejo, MD.
Hantavirus does not usually pass person-to-person. The only type that has been thought to do that is the Andes virus. In one outbreak with the Andes virus in 2011, some close contacts, such as spouses who shared a bed during the febrile illness, and hospital contacts, such as providers involved in patient care, resulted in infection. However, in another outbreak with the Andes virus in 2018, there was no nosocomial transmission, even in patients who had undergone high-risk procedures, including but not limited to intubation.4 For cases of presumed transmission, significant exposure to bodily fluids, typically saliva, from an infected person during the prodromal phase of the illness was likely involved. However, as mentioned above, documentation of person-to-person transmission is complicated by the long latency phase of the virus.5 Case tracking of the outbreak on a cruise ship in 2026 has generated some additional cases of person-to-person transmission. The long latency of this illness means at the time of this writing there is still uncertainty about the details of person-to-person spread during this outbreak, but extended contact or shared living spaces may be an important factor.
The clinical features of Hantavirus infection mirror typical symptoms of inflammation and viral illness. Fever, myalgias, backache, and headaches are common, and there can be associated abdominal pain severe enough to mimic an acute abdomen; there are reports of patients having appendectomies and later being diagnosed with Hantavirus.2,6 In addition, both HCPS and HFRS can progress to thrombocytopenia, oliguria, kidney injury, and respiratory failure.3 HCPS is more likely to progress to severe respiratory failure. Viral particles are at the highest concentration in blood, but can be in other bodily fluids. Thus, there is at least some risk, however small, of nosocomial viral transmission that could result in severe injury. As such, these healthcare exposures should be taken seriously and risk mitigation strategies employed. Testing for Hantavirus infection is possible using PCR techniques. There are no approved clinical PCR tests for Andes virus type in the United States, but these are being developed.7 Later in the course of illness, antibody-based tests may be useful. While there are no approved vaccines in the United States, there are moderately effective vaccines targeted to HFRS in Korea and China.8 In many locations, Hantavirus infection needs to be reported to the local public health officers. Due to the seriousness of the illness, patients with suspected or confirmed Hantavirus infection will likely benefit from evaluation by the infectious disease team and hospital infection control.
Given that Hantaviruses are enveloped and of similar size (80-110 nm) to the SARS-CoV-2 virus, similar protective strategies should be employed.9 A demonstration of the following strategies can be found at: https://www.youtube.com/watch?v=C2pT1jg5QUs and at https://www.apsf.org/news-updates/optimizing-infection-control-and-or-management-during-the-covid-pandemic/. Some institutions are treating this with the highest level of precaution, as is done for other hemorrhagic fevers, such as Ebola or Marburg.
Both in the operating room and in the intensive care unit, anesthesia professionals should use appropriate personal protective equipment (PPE) to protect themselves when treating patients with known or suspected Hantavirus infection. The authors advocate for N95 masking or powered-air purifying respirator (PAPR) use during airway management and any aerosol-generating procedures for these patients.10 Eye protection is recommended, if the eyes are not otherwise protected. Use of surgical and N95 double masking or PAPR may not intercept all viral particles due to their small size. As such, personal use of nasal povidone iodine in conjunction with masks can be considered.9,11 Application of nasal povidone iodine could be augmented with a gargle of dilute 1:10 povidone iodine in water.12
To prevent the spread of the virus particles, close attention to environmental cleaning during the anesthesia case, and between cases, is warranted. Hand hygiene should be used to prevent the spread of viral particles. Alcohol-based hand sanitizers should be in close proximity to the anesthesia professional and clean and dirty areas within the anesthesia workspace should be designated. Following induction of anesthesia, a top cleaning approach of the anesthesia machine and equipment with quaternary ammonium compound and alcohol wipes should be used, and needleless injection ports should be disinfected prior to access.8 Between cases, a terminal-level operating room cleaning is indicated. If available, augment terminal cleaning with UV-C irradiation using evidence-based approaches.13
Unfortunately, there are no standard viral treatments for Hantavirus infections. Several older viral treatments, including ribavirin, have been studied, but they have not been shown to be effective. A combination of ribavirin and favipiravir has demonstrated in-vitro activity against the virus, worthy of additional study.14 As such, supportive care is generally recommended until convalescence. In severe cases of respiratory failure, extracorporeal membrane oxygenation could be considered as a bridge to recovery.15
There are no published recommendations addressing elective surgeries for patients who have been exposed to Hantavirus but have not yet become ill. Because most cases are zoonotic and the time of exposure is only determined in retrospect, there are no guidelines for how to proceed if a patient has been exposed but is not yet ill. Anesthesia professionals could consider delaying elective surgeries for patients who have a known exposure until after the latent period has elapsed, thirty-nine days. Patients who are acutely sick from Hantavirus should delay elective surgery until they have returned to full health, which may take months. For emergent procedures in patients with Hantavirus, considerations should be made for appropriate risk mitigation for both patients and operating room staff. During emergency surgery, anesthesia professionals should plan for excess bleeding due to thrombocytopenia and coagulation system dysfunction. Postoperatively, it is reasonable to consider whether patients will need to recover in a room with appropriate isolation and a negative pressure environment.
Hantavirus infection produce severe disease and mortality. While there are no current evidence-based guidelines about how to proceed with the perioperative care of these patients, elective surgery should be delayed if possible and patients who are acutely ill should have surgery postponed until full recovery has been made. Anesthesia and critical care professionals should take precautions, including use of eye protection and N95 masks or PAPRs.
Jonathan E. Charnin, MD FASA is an assistant professor of anesthesiology at Mayo Clinic, Rochester, Minnesota, USA.
Brendan T. Wanta, MD is an assistant professor of anesthesiology at Mayo Clinic, Rochester, Minnesota, USA.
Randy W. Loftus, MD is a professor of anesthesiology at Mayo Clinic, Rochester, Minnesota, USA
Jonathan Charnin and Brendan Wanta have no conflicts of interest. Randy W. Loftus has shares in RDB Bioinformatics, a company that owns OR PathTrac. There are no relevant conflicts related to this article.
Acknowledgements: The authors would like to acknowledge the help of Arney Abcejo, MD.
REFERENCES
- Basu MF, R. Hantavirus crops up on a cruise ship — what scientists are watching. Updated May 4, 2026. Accessed May 7, 2026. Available at: https://www.nature.com/articles/d41586-026-01450-7
- Vial PA, Ferres M, Vial C, et al. Hantavirus in humans: a review of clinical aspects and management. Lancet Infect Dis. 2023;23(9):e371–e382. PMID: 37105214
- Riquelme R. Hantavirus. Semin Respir Crit Care Med. 2021;42(6):822–827. PMID: 34918323
- Martinez VP, Di Paola N, Alonso DO, et al. “Super-Spreaders” and Person-to-Person Transmission of Andes Virus in Argentina. N Engl J Med. 2020;383(23):2230–2241. PMID: 33264545
- Toledo J, Haby MM, Reveiz L, Sosa Leon L, Angerami R, Aldighieri S. Evidence for Human-to-Human Transmission of Hantavirus: A Systematic Review. J Infect Dis. 2022;226(8):1362–1371. PMID: 34515290
- Lim SC, Lee YM, Kim CM, Yun NR, Kim DM. Acute Appendicitis Associated with Hantaan Virus Infection. Am J Trop Med Hyg. 2021;105(3):801-806. PMID: 34228635
- Mullin, Emily. Inside the Race to Develop a Test for the Rare Andes Hantavirus. Wired. May 13, 2026. Accessed May 7, 2026. Available at: https://www.wired.com/story/race-to-develop-andes-hantavirus-test/
- Chai S, Wang L, Du H, Jiang H. Achievement and Challenges in Orthohantavirus Vaccines. Vaccines (Basel). 2025;13(2):198. PMID: 40006744
- Dexter F, Parra MC, Brown JR, Loftus RW. Perioperative COVID-19 Defense: An Evidence-Based Approach for Optimization of Infection Control and Operating Room Management. Anesth Analg. 2020;131(1):37–42. PMID: 32217947
- Siegel JD, Rhinehart E, Jackson M, Chiarello L, Health Care Infection Control Practices Advisory Committee. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. Am J Infect Control. 2007;35(10 Suppl 2):S65–164. PMID: 18068815
- Knight CA, Stanley WM. The Effect of Some Chemicals on Purified Influenza Virus. J Exp Med. 1944;79(3):291–300. PMID: 19871371
- Guenezan J, Garcia M, Strasters D, et al. Povidone Iodine Mouthwash, Gargle, and Nasal Spray to Reduce Nasopharyngeal Viral Load in Patients With COVID-19: A Randomized Clinical Trial. JAMA Otolaryngol Head Neck Surg. 2021;147(4):400–401. PMID: 33538761
- Gibbons S, Dexter F, Loftus RW, et al. An Analysis of Ultraviolet-C Light Irradiation in Reducing Bacterial Contamination of the Anesthesia Work Area. Anesthesiology. 2024;141(4):793-796. PMID: 39254537
- Mayor J, Engler O, Rothenberger S. Antiviral Efficacy of Ribavirin and Favipiravir against Hantaan Virus. Microorganisms. 2021;9(6):1306. PMID: 34203936
- Wernly JA, Dietl CA, Tabe CE, et al. Extracorporeal membrane oxygenation support improves survival of patients with Hantavirus cardiopulmonary syndrome refractory to medical treatment. Eur J Cardiothorac Surg. 2011;40(6):1334-1340. PMID: 21900022
