To the Editor
Loss of endotracheal tube cuff pressure compromises secure airway and can increase aspiration risk. Common explanations for apparent endotracheal cuff pressure loss include tube migration after changes in patient positioning leading to partial extubation, cuff trauma from direct patient or laryngoscope contact, and product defects such as pilot balloon valve incompetency.
This case illustrates an unexpected product defect in the pilot line of the Single Use ILMA-Fastrach™ (The Laryngeal Mask Airway Company, San Diego, California) silicone endotracheal tube. This is the first case report documenting this remediable defect, thereby addressing a meaningful airway device knowledge gap.
A 31-year-old man with a BMI of 23 kg/m2 and no aspiration risk factors presented for incision and drainage of a right-hand abscess. Prior to intubation, silicone tube cuff patency was confirmed via brief air insufflation followed by rapid deflation, and the tube was lubricated and passed through the ILMA. General anesthesia was induced using fentanyl and propofol, followed by blind, facile first pass endotracheal intubation via the Single Use ILMA-Fastrach™. The silicone tube was secured at a depth of 25 cm at the ILMA airway tube 15-mm connector. The ILMA cuff was deflated after confirmation of consistent, spontaneous rhythmic end-tidal CO2 return.
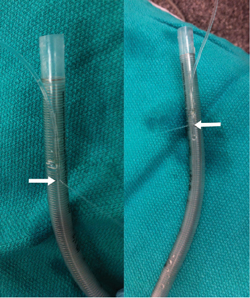
Figure 1.Saline injected into the pilot balloon is seen ejecting from the pilot line defect. [Arrows]
After uneventful completion of surgery and airway device removal, the silicone tube cuff was inflated with normal saline in an attempt to localize the cuff leak. A defect was noticed in the outer pilot line at the point where it invaginates into the endotracheal tube [Figure 1].
Loss of endotracheal tube cuff pressure can be a concerning event for an anesthesia provider.Exchanging an endotracheal tube intraoperatively can involve considerable risk, especially if a patient has a difficult airway, is positioned non-supine, or if the surgical field limits access to the tube. Pragmatic solutions to temporarily maintain cuff pressure and avoid airway device exchange have been previously reported. These include use of continuous insufflation of the endotracheal tube cuff with air, cuff inflation with a viscous liquid such as normal saline or lidocaine jelly, and use of a 3-way stopcock to fix a leaky pilot balloon.1-4
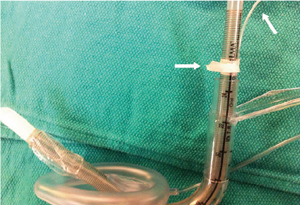
Figure 2.The ILMA silicone tube utilizes a short exterior pilot line [Arrows], thereby affording access to and sealing of the defect (26 cm) while potentially maintaining tracheal intubation (25 cm).
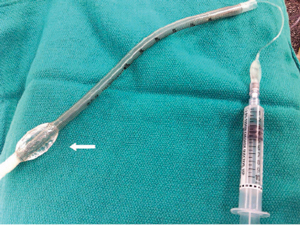
Figure 3. The silicone tube cuff can be filled with saline, circumventing the pilot line defect and maintaining cuff patency. Note that the pilot balloon cuff remains deflated.
When attempting to localize the source of an endotracheal tube cuff leak, it is possible to overlook pilot line inspection given the rarity of such defects. Upon removal this pilot line defect was readily apparent by injecting saline into the pilot balloon. Had the pilot line leak been localized intraoperatively, various options would have existed to maintain cuff patency. For example, leakage from the pilot line defect could have been sealed using tape. This is possible with the ILMA silicone tube since it has an exterior pilot line that invaginates 26 cm distal from the endotracheal tube tip [Figure 2]. Note that this can readily be accomplished with the silicone tube remaining in the trachea. Alternatively, the defect could have been circumvented by inflating the cuff with normal saline [Figure 3]. In short, localization of the defect to the pilot line can circumvent endotracheal tube replacement with the intention of secure airway maintenance.
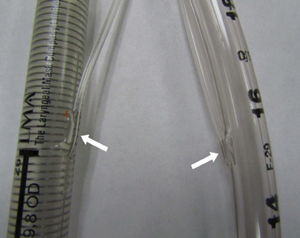
Figure 4. The pilot line of the ILMA silicone tube invaginates into the endotracheal tube more distally (26 cm from the tip) than a standard endotracheal tube (15 cm – Sheridan/CF®
Endotracheal Tube, Hudson RCI®, California). Differences exist in protection at the junction where the pilot line enters the main endotracheal tube [Arrows], with the standard tube employing less pliable material.
In conclusion, this pilot line defect is easily detectable and repairable in situ, allowing for secure airway preservation and avoiding the risk of endotracheal tube exchange.
Kenneth N. Hiller, MD
Assistant Professor of Anesthesiology
Director of Post Anesthesia Care Unit
The University of Texas Medical School at Houston
Hassan Aijazi, MBBS
The University of Texas Medical School at Houston
Department of Anesthesiology
References
- Schubert A, Von Kaenel W, Ilyes L. A management option for leaking endotracheal tube cuffs: use of lidocaine jelly. J Clin Anesth 1991;3:26-31.
- Rudlof B, Lauterbach C. Intracuff saline infusion for the short-term repair of an endotracheal tube cuff leak. Anesthesiology 1999;90:1801.
- Ho AM, Contardi LH. What to do when an endotracheal tube cuff leaks. J Trauma 1996;40:486-7.
- Sprung J, Bourke DL, Thomas P, Harrison C. Clever cure for an endotracheal tube cuff leak. Anesthesiology 1994;81:790-1.
- Karim YM, Swanson DE. Comparison of blind tracheal intubation through the intubating laryngeal mask airway (LMA Fastrach™) and the Air-Q™. Anaesthesia 2011;66:185-90.
- Aikins NL, Ganesh R, Springmann KE, Lunn JJ, Solis-Keus J. Difficult airway management and the novice physician. J Emerg Trauma Shock 2010;3:9-12.
- Wiesel S, Warm T. Fastrach uses a low-volume, high-pressure cuff for the endotracheal tube system. Anesthesiology 1999;91:592-5.
- Suneel PR, Koshy T, Unnikrishnan KP. High cuff pressure in the silicone endotracheal tube of the LMA-Fastrach: implications for patient safety. J Clin Anesth 2011;23:666-7.
