To the Editor:
Airway suctioning is usually performed by introducing a suction catheter into the endotracheal tube after disconnecting the patient from the ventilator. It can also be accomplished with a closed suctioning system (CSS) included in the ventilator circuit, which allows the introduction of suction catheter into the airway without disconnecting the patient from the ventilator. Closed suctioning technique facilitates continuous mechanical ventilation and oxygenation during the suctioning event. CSS has some advantages compared to the conventional, open-suction technique. It can be helpful in limiting environmental, personnel, and patient contamination and in preventing the loss of lung volume and the alveolar derecruitment associated with standard suctioning in severely hypoxemic patients. The use of closed suction is suggested for adults requiring high FiO2, or PEEP, or at risk for lung derecruitment, and for neonates.1
A patient on mechanical ventilation in our intensive care unit with CSS (Portex® SuctionPro 72™, Dual Lumen Closed ventilation suction catheter with T connector) developed gradual (over a period of half an hour) desaturation while being ventilated in synchronized intermittent mandatory ventilation mode. Common causes for hypoxia in a patient on mechanical ventilation related to endotracheal tube and breathing circuits like kinking, displacement, disconnections, leaks and obstruction, pneumothorax were ruled out by bedside clinical examination. A small quantity of clear aspirate was observed on endotracheal suction. While the cause for desaturation was being actively searched for, we noticed the catheter mount filled with fluid. Upon examination of the CSS it was noticed that the nursing staff had kept connected a 500 ml Normal Saline (NS) bottle to the saline port of CSS (Figure 1) with the intravenous infusion set "on", suction port kept connected to the central suction and thumb control valve in "off" position. NS drops were seen being slowly infused into the breathing circuit. NS was immediately disconnected from the CSS and the catheter mount was drained of fluid. Oxygen saturation improved steadily over the next hour and the patient was subsequently discharged from the ICU after recovery.
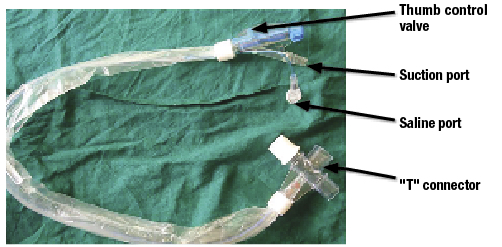
Closed suction catheter that was misused resulting in oxygen desaturation.
In an apparent attempt to reduce the overall time and number of tasks required to perform endotracheal suctioning, the nursing staff had kept the NS connected to the saline port of the CSS. The one-way valve in the saline port is designed to prevent inadvertent saline aerosolization.2 By attaching the intravenous infusion set firmly to the irrigation port, the one-way valve was in "open" position allowing sustained irrigation of saline leading to flooding of the airway as the infusion set was also kept "on."
Even if it is slightly labor-intensive and time consuming to irrigate saline using a saline filled syringe, saline should not be kept connected to the CSS through an intravenous infusion set. There is no instruction in the product insert regarding how to irrigate or a warning regarding the possibility of inadvertent aerosolization of saline if fluid is kept connected to the irrigation port. This incident is reported to alert the caregivers, especially the intensive care specialists and nursing staff working in intensive care units, about this potential complication associated with CSS.
Harihar V. Hegde, MD
Vinayak B. Nayak, MBBS
Dept. of Anaesthesiology, SDM College of Medical Sciences and Hospital, Sattur, Dharwad, India.
Conflicts of interest and financial support: There are no conflicts of interest involved in this report.
References
- Restrepo RD, Brown JM 2nd, Hughes JM. AARC Clinical Practice Guidelines. Endotracheal suctioning of mechanically ventilated patients with artificial airways 2010. Respir Care 2010;55:758-64.
- http://bcove.me/noraas7w Accessed May 5, 2015.
