Episode #36 Detecting Potential Failures and Improving Patient Safety
March 16, 2021
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Today, we review the article, “Proactive Perioperative Risk Analysis: Use of Failure Mode and Effects Analysis (FMEA)” by George Tewfik, MD, MBA, CPE from the February 2021 APSF Newsletter. Thank you to George Tewfik for contributing to this show by sharing his insights into this area. You can find the article here. https://www.apsf.org/article/proactive-perioperative-risk-analysis-use-of-failure-mode-and-effects-analysis-fmea/
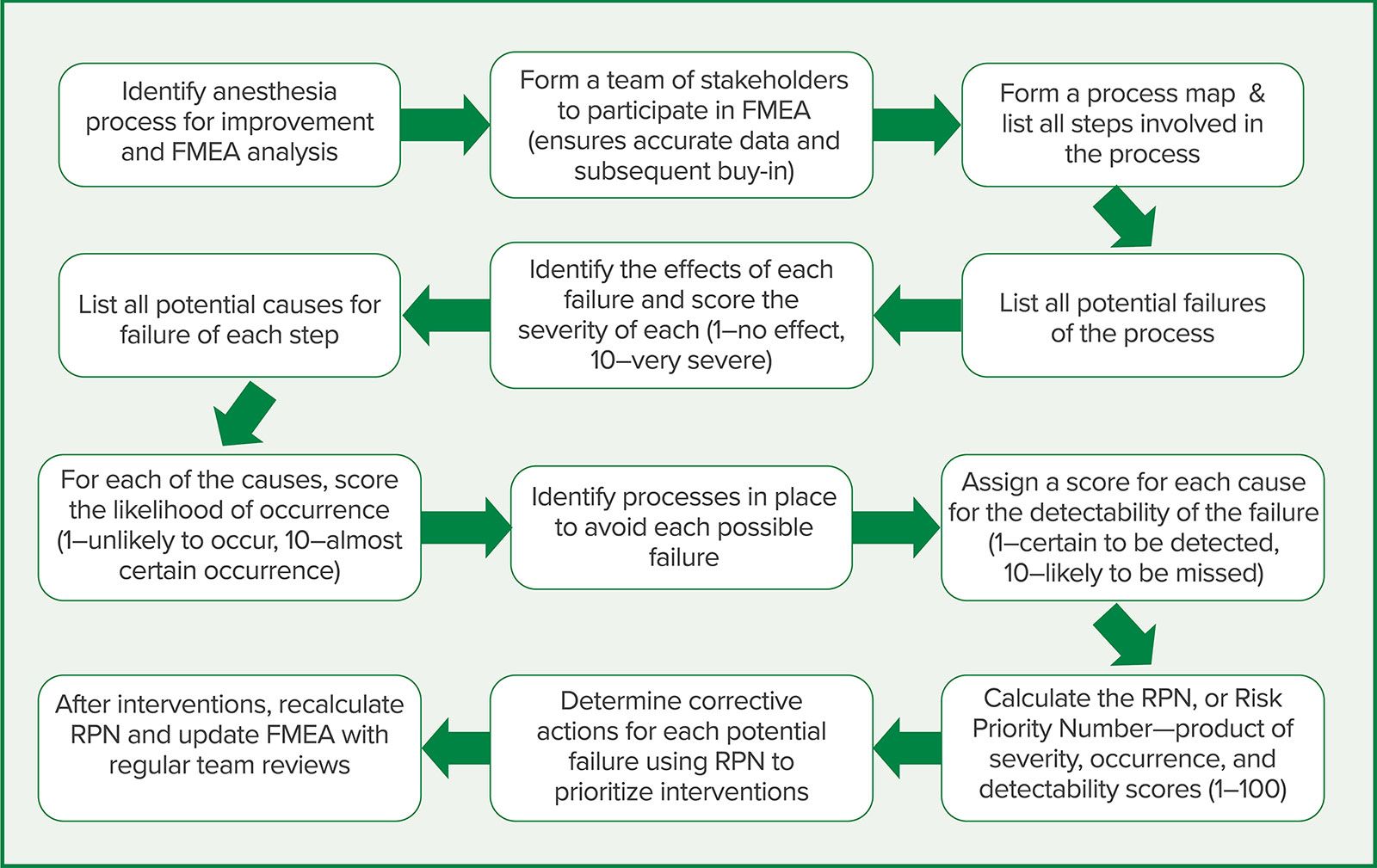
Figure 1: Application of FMEA and the steps involved for an anesthesia process.
Here is a link to the Healthcare Failure Mode and Effects Analysis site. https://www.patientsafety.va.gov/docs/hfmea/HFMEAIntro.pdf
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be apart of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
© 2021, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel and I am your host. Thank you for joining us for another show. Today, we are diving back into the February 2021 APSF Newsletter to learn all about Failure Mode and Effects Analysis and how this method can be used to improve anesthesia patient safety as well as efficiency.
Before we dive into today’s episode, we’d like to recognize Medtronic, a major corporate supporter of APSF. Medtronic has generously provided unrestricted support as well as research and educational grants to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Medtronic – we wouldn’t be able to do all that we do without you!”
I am so excited to review this article especially because we will be hearing for the author, George Tewfik. I am going to let him introduce himself now.
[Tewfik] Hi, my name is George Tewfik, I am an assistant professor of Anesthesiology at Rutgers New Jersey Medical School and I am the director of quality assurance for the department.
[Bechtel] To get started, I asked Tewfik why he wrote this article. Let’s take a listen to what he had to say.
[Tewfik] I wrote about proactive error analysis in anesthesiology because it is critically important to remember that quality assurance is not just about addressing mistakes after they happen. It is also about analysis systems and process to ensure the most optimal performance of a perioperative service. Quality assurance can’t be a punitive and adversarial process and requires buy-in from numerous services and personnel.
[Bechtel] I hope you are ready to learn more about proactive error analysis. So, let’s get into the article and then we will hear more from Tewfik soon. To follow along with us, head over to the APSF website and click on the Newsletter heading. First one down is the current issue. Then scroll down. Our featured article today is the 6th article down. We need to start with some definitions because you may not have heard of failure mode and effects analysis or FMEA. So, what is it? Tewfik tells us that FMEA is a tool for process analysis and it is used in high risk industries to evaluate manufacturing or assembly process. This tool provides information by breaking down a specific process into the individual steps to evaluate for steps that are at risk for failure. As part of this process, each step is given a risk priority number or RPN depending on the required resources including time, money, and manpower and this helps to determine how to use resources efficiently and effectively to make the biggest impact. So far, I haven’t mentioned anesthesia or medicine, but by diving further into the article we will see how this process can be applied to perioperative processes leading to increased efficiency and improved anesthesia patient safety. If you haven’t heard of FMEA yet, you may be familiar with other methods to improve patient safety including root cause analysis or RCA and the Safety Assessment Code or SAC. So, what data do we have that patient safety initiatives actually lead to safer anesthesia care? The Department of Veterans Affairs patient safety program has been in place for 30 years and proactive analysis has led to a decrease in MRI hazards and cardiac pacemaker malfunction. More data supporting the use of proactive analysis comes from the Safer Patients Initiative in the United Kingdom which led to decreased adverse events from 7% down to 1.5% per 1,000 patient days in the first year of the program.
Now, let’s take a look at FMEA specifically and the good news is that this is a success story. FMEA has been used to make heparin administration to patients safer. In one study at a 367-bed academic pediatric hospital, unfractionated heparin administration was found to be associated with hundreds of potential errors from hundreds of causes and the opportunity for numerous countermeasures to improve safety. Some of these potential errors included mathematical errors, unknown requirements for administration, incorrect timing of administration, challenges with the hospital electronic medical record, poor patient education, and the ability to administer incorrect dosages. The steps in administration were assigned appropriate risk priority numbers and countermeasures were applied to the highest RPN with improved safety of heparin administration.
Now, I have just mentioned one area where FMEA was applied with improve processes and patient safety. There are many other areas associated with perioperative and anesthesia patient care where FMEA may be used. There is a chart in the article that highlights these areas including the following:
- Medication Safety including allergy avoidance, ordering, administration, and post-administration monitoring.
- Equipment Safety including routine check, equipment failure, availability, and emergency equipment
- Clinical Care including airway management, avoiding laryngospasm, prevention of PONV, perioperative pain management, and prevention of surgical site infections.
- Hospital Processes including OR scheduling, patient transport, bed management, and OR turnover
- Preoperative Workup including case booking, preop evaluation booking, consultations, labs and studies, and anesthesia evaluation
- PACU processes including patient monitoring and evaluation as well as PONV and pain management
- Regional Anesthesia including consultation and scheduling, equipment preparation, and catheter management
Given all these areas where FMEA may be used, there are not very many studies on this method for improving anesthesia patient safety. Past studies have been completed looking at anesthesia equipment maintenance and repair, medication safety in pediatric anesthesia, and propofol administration in endoscopy.
Now, that we know where FMEA has been used and studied in the past and the potential for its use in the future, let’s talk about the steps for conducting a FMEA. There is a figure in the article that I will include in the show notes as well. Lace up your walking or running shoes and let’s get ready to take some steps.
Step 1 involves identifying the process that needs to be optimized and improved using a FMEA.
Step 2 involves forming a team with the relevant stakeholders to participate in the FMEA.
Step 3 involves drawing the process map and listing all of the steps in the process
Step 4 involves creating a list of all the potentials failures during the process
The next step is identifying the effect of each potential failure and assigning a severity score from 1-10.
Now, we are on to step 6 which involves developing a list of all the potential causes for failure at each step.
Moving on to the next step involves scoring the likelihood of each potential cause of occurring from 1-10.
Step 8 involves identifying the processes that exist to avoid each potential failure.
Step 9 involves scoring each cause for the ability to detect the failure from 1 certain to be detected to 10 for likely to be missed.
For the next step, we can finally assign the RPN or Risk Priority Number which is the product of the severity, occurrence, and detectability scores and falls between 1-100.
Only 2 more steps left which involve creating countermeasures for each potential failure and prioritizing the interventions depending on the RPN and then finally after implementation, it is important update the FMEA including recalculating the RPN.
As you can see it is not a simple process and there are many steps involved, but the impact is to help improve efficiency as well as patient safety. In the article, Tewfik provides an example for this method being used to evaluate pre-anesthesia evaluations at his institution for outpatients who were referred to the pre-admission testing clinic by the surgery team. Remember, the first step is to outline each step of the process. For this FMEA, the first step was booking the appointment in the clinic and other steps included patient reminder, patient arrival to appointment, appropriate staff available at the appointment, patient history and physical exam, labs, consults, and referrals leading up to the last step which is providing patient instructions for the day of surgery and there is a chart in the article that represents a simple version of the FMEA. The chart also provides the necessary information to see how the RPN was determined for each step. By looking at the chart, you can see that the areas with higher RPN scores with a higher need for intervention and improvement include patient presenting for the appointment, having staff available, and consults. Even at this stage before any interventions are made, the FMEA has provided vital information about which areas to focus on to have the biggest impact on improved patient safety and often efficiency as well. At the authors institution, the countermeasures included the following:
- Improved patient transport to the appointments with confirmation of transportation availability at the time of booking
- Assigning an anesthesia resident to the pre-anesthesia evaluation clinic to help ensure that staff is available to evaluate patients. There are also 2 nurse practitioners who work in the pre-anesthesia clinic as well.
- Planning for telemedicine visits to replace in-person evaluations when appropriate
- And, improved communication between consultant services by scheduling appointments through the pre-anesthesia clinic rather than relying on the patients to schedule with a process for the anesthesia and surgery teams to follow-up with the consultants prior to the day of surgery.
After completing the FMEA and starting to implement interventions to address potential failures, it is important to repeat the FMEA analysis and re-score the RPN to monitor for improvement and this can provide additional information about the next steps to take to continue to improve the overall process.
This sounds like a wonderful tool that we should be using more in perioperative medicine. However, it is not widely used at this time which may be due to requirement for a multidisciplinary team to meet and determine each step of the process and work through it until the RPN score for each process is calculated and very detailed information must be gathered in order to complete the FMEA. Another limitation of FMEA use for process improvement in healthcare may be the equal weight given to occurrence, severity and detectability with difficulty assessing the 3 risk factors. Due to these limitations, the National Center for Patient Safety developed the Healthcare Failure Mode and Effects Analysis and this has been adopted by the VA National Center for Patient Safety. Changes to this method include combining detectability and the critical nature of the potential failure into a decision-making algorithm which will ultimately yield a hazard score rather than an RPN. These modifications have helped to simplify the process, especially when deciding on corrective actions and order of implementation. It would be wonderful if every hospital system could use the FMEA already completed by the author at his institution on the pre-anesthesia evaluation process, but since there are different and unique process steps at every hospital, the FMEA needs to be individualized for each hospital system. Perhaps, at your hospital there are no anesthesia residents to help staff the pre-anesthesia clinic which would create a different process with different interventions.
Despite these limitations and the work that must go into using FMEA, this is an important tool for healthcare professionals interested in patient safety as well as efficiency. The information provided from the FMEA can be used to help direct resources, which may be limited at times, towards interventions that will have the most impact on preventing process failures. This is a team approach with a built-in review system to re-evaluate the processes and the impact of the interventions with re-direction of resources towards the next set of interventions so that there continues to be a big impact and improved process. Tewfik concludes the article with this call to action: “This author strongly recommends its use in anesthesiology and perioperative medical processes to assist in improving quality and safety via a systematic process to identify where attention and resources will be most effective.”
Before we conclude the show for today, I asked Tewfik another question about what he hopes to see going forward related to adverse events and anesthesia patient safety. Let’s take a listen to what he had to say.
[Tewfik] Moving forward, I hope to continue to research and publish regarding adverse event analysis. How we analysis potential modes of failure in perioperative medicine is not a one size fits all model. Educating anesthesia personnel on the different systems and pathways available will hopefully enable each group or department to find a system that works for their institution.
[Bechtel] Thank you Tewfik for contributing to the show today. What system do you use for adverse event analysis at your institution? This is such an important area to evaluate the potential for threats to anesthesia patient safety and take action to help improve safety.
If you have any questions or comments from today’s show, please email us at [email protected].
Visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today. Don’t forget to subscribe to the podcast through iTunes or your favorite podcast app and we would love it if you could share this podcast with all of your work colleagues, friends, and family and don’t forget to leave us a review.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2021, The Anesthesia Patient Safety Foundation
