Episode #301 Pro-Social Operating Rooms
April 8, 2026
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article is “Reduce Burnout, Improve Safety and Efficiency: Consider Prosocial Behavior” by Jeffrey Feldman, MD, MSE, FASA; Ramona Houmanfar, PhD; Mary Fearon, RN, MSN; John M. Flynn, MD; Jeffrey B. Cooper, PhD;, Stuart Libman, MD; Caoimhe Duffy MD MSc CPPS FCAI; Lisa Spruce, DNP, RN, CNOR, CNS-CP, EBP-C, APRN, FAAN; Della Lin, MS, MD, FASA. This is Part 2 of our two-part series.
Check out Figure 1 in the article to learn more about the ACT Matrix that we talked about on the show today.
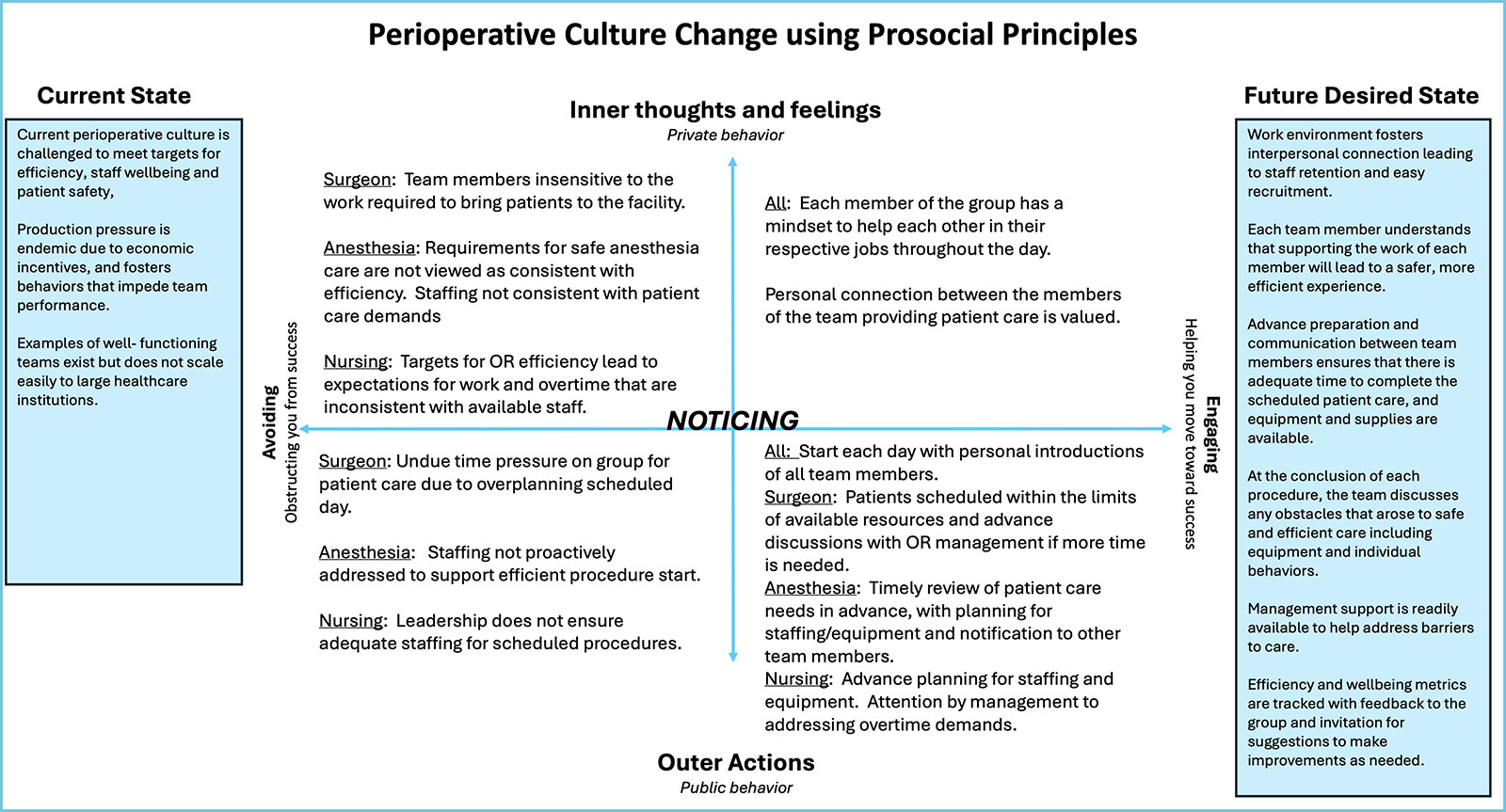
Figure 1: ACT Matrix applied to a procedural team helps to understand the behaviors required to move from the current state to a more desired future state. Specific behaviors move the individual or group towards the desired future state (engaging) or away from the current state (avoiding) as indicated by the horizontal axis. The vertical axis indicates differences between “Outer” or observable behaviors and “Inner” behaviors or what we experience. Avoiding-behaviors are typically self-interested; engaging behaviors are prosocial, intended to foster the group mission. The individual action of NOTICING these behaviors and developing the psychological flexibility to replace avoiding behaviors with engaging behaviors is central to ACT training. Special thanks to Dr. Kevin Polk and colleagues for their original formulation. (Adapted with permission from Paul Atkins.)
Thank you so much to the authors for contributing to the show and for your hard work on this project. For more information about prosocial behaviors, check out the website here: https://www.prosocial.world/
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2026, The Anesthesia Patient Safety Foundation
Opening clip: [Bechtel] “So, how do we change the culture in the operating room environment? We need to recognize the limitations of the existing culture and the potential value for making the change. Perhaps, the current staffing shortages leading to burnout syndrome in healthcare can be a motivating factor. Plus, with increasing efficiency goals, prosocial behaviors and teamwork can bring groups of people together to help meet these goals. The authors tells us that the potential value of prosocial change is to create a culture that fosters highly functional teams that maximize efficiency and derive job satisfaction from collegial relationships and collectively achieving shared goals. It is easy to see why this is a desirable goal, but the path to success in procedural areas in healthcare is not defined and new methods are needed.”
Hello and welcome back to the Anesthesia Patient Safety Podcast. I’m your host, Alli Bechtel. We are back talking about prosocial behaviour again today. This is the second part of our 2-part series. Remember, prosocial behaviour involves voluntary actions made for the benefit of others including kindness, cooperation, and gratitude. We often talk about the risks and benefits in medicine. The benefits of prosocial behaviours include reduced cognitive load, improved communication, decreased clinician burnout, improved operational resilience, and enhanced patient safety. The only risk is not including prosocial behaviour in your day to day.
Before we dive further into the episode today, we’d like to recognize BD, a major corporate supporter of APSF. BD has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, BD – we wouldn’t be able to do all that we do without you!”
Our featured article is “Reduce Burnout, Improve Safety and Efficiency: Consider Prosocial Behavior” by Jeffrey Feldman and colleagues from the February 2026 APSF Newsletter. To follow along with us, head over to APSF.org and click on the Newsletter Heading. The first one down is the current newsletter. Then, you can scroll down until you get to our featured article and I will include a link in the show notes as well.
Let’s pick up right where we left off, with the Core Design Principles for Successful Group Collaboration. This model comes from Elinor Ostrom’s research on group collaboration for which she won the 2009 Nobel Prize in Economics. Following up, David Sloan-Wilson generalized the Core Design Principles and applied them to understanding any group where there is a shared common goal. This is what we have in the operating room, a group with a shared common goal. Table 1 in the article provides a list of the 8 Ostrom Core Design Principles, the generalized principles, and the adaptive impact. Let’s review it now.
The 8 Ostrom Principles include:
- Clearly defined boundaries
- Proportional equivalence of benefits and costs
- Collective choice arrangements
- Monitoring
- Graduated sanctions
- Conflict resolutions and mechanisms
- Minimal recognition of rights to organize
- And Polycentric governance.
Here are the generalized prosocial principles:
- Shared identity and purpose
- Equitable distribution of costs and benefits
- Fair and inclusive decision-making
- Monitoring agreed behaviors, which means transparency
- Graduated response to helpful and unhelpful behaviors
- Fast and fair conflict resolution
- Authority to self-govern
- And collaborative relations with other groups.
And for the third column, the adaptive impacts include the following:
- A group that works for all:Defines the group and its culture as purposeful, equitable with a power arrangement appropriate for the mission.
- All working for the group:Ensures effectiveness within groups by utilizing reciprocity, reputation, and trust to balance individual and collective interests.
- Working with other groups:Ensures effectiveness between groups by balancing interests and supporting shared power.
Before we continue with the article, we are going to hear from one of the authors. Let’s take a listen now.
[Ramona] “Hi, my name is Ramona. I’m a professor of psychology and director of Behavior Analysis program at the University of Nevada Reno.”
[Bechtel] I asked Ramona what got her interested in this topic. Here’s her response.
[Ramona] “ All of these topics, uh, speak directly to my conceptual and research interests, uh, over the years, uh, with a focus on scientific, behavioral, scientific account of wellbeing and organizations and beyond.
It also speaks to my 14 years of interdisciplinary collaboration with leadership teams at the University of Nevada Reno School of Medicine. Throughout the years, we’ve been able to institutionalize assessment measures of burnout and psychological flexibility and develop curriculum referred to as acceptance and commitment training curriculum at UNR Med that have allowed for us to determine a longitudinally speaking, uh, the impact of exposure to the curriculum by medical students on their measures of burnout, psychological flexibility, levels of cooperation, plus academic performance and interprofessional communication.”
[Bechtel] Ramona also shares what she hopes to see going forward.
[Ramona] “ I’m looking forward to contributing to this collective effort by bringing to bear what I’ve learned, uh, through my interdisciplinary collaborations, uh, with high performance groups in the areas of systematic enhancement of psychological safety and pro-social behaviors with an eye on, uh, patient safety, in this case, in, uh, perioperative, uh, processes.
This also includes, uh, what. We can facilitate in terms of leadership buy-in, and promotion of psychological flexibility and post social practices at the large scale levels in medical settings and beyond.”
[Bechtel] Thank you so much to Ramona for contributing to the show today.
We can use the CDPs to evaluate how well the team from the vignette that we read last week is likely to function as a group. This framework can help to identify opportunities for improvement. Let’s take a look at Table 2 in the article for a example of how the CDPs can be applied to the problem of efficiency in the operating room by breaking down the vignette that we talked about last week.
First, is there shared identify and purpose? The positive contributor is a commitment to the patient’s safety and outcome and the negative contributor is the questionable shared team identity where efficiency and safety goals are in conflict with each other.
Next, is there equitable distribution of contributions and benefits? On the positive side is the shared benefit of employment while on the negative side there are inequalities in the team including hierarchy and autonomy as well as the surgeon’s work extending beyond the procedure.
The 3rd question, is there fair and inclusive decision-making? The positive contributor is the morning huddle was used for the team to review the needs of the day. On the flips side, the procedures were planned without input from the rest of the team.
The next CDP is monitoring of agreed behaviours. The positive contributor is that efficiency metrics are usually tracked in the operating room environment, but on the negative side, unacceptable behaviours are not well defined nor consistently monitored.
Moving on to gradual responding to helpful and unhelpful behavior. The positive contributor is the emphasis on psychological safety to empower all personnel and the negative contributor is that there is no accepted standard for responding to behaviours that impede patient care goals.
Asking the question, is there fast and fair conflict resolution? It is a negative continuation when there is no formal process for addressing staff conflicts that impede team performance.
The next CDP that we are looking at in this example is the authority to self-govern. On the positive side is that operating room teams typically control the activities of the day without close management of tasks and patient flow while on the negative side, OR teams have limited ability to impact system problems that impede performance.
The 8th CDP is collaborative relations with other groups and on the negative side is the communication between the intra-procedure team and the pre- and post-procedure teams are typically not well integrated.
As we can see, there are many opportunities for improvement for our sample OR team.
One of the benefits of prosocial behaviors is improved well-being for team members. We can determine the level of well-being by measuring the coercive control in one’s environment. In other words, does an individual have opportunities to influence their environment and have access to positive consequences? Let’s return to the original vignette where there are coercive forces acting on the team members from production pressure and hierarchical relationships. We can break it down further. The nurse has limited opportunities to influence the environment due to limitations from training needs for the scrub tech. The anesthesiologist is limited by needing to care for another patient and the nurse anaesthetist is limited by their temporary status. The surgeon is limited by needing to use their block time to provide timely are for patients. Overall, the group likely has the shared goals for safe and effective care for the patients completed in a timely fashion, but there are many factors that are working in opposition to these goals.
What if we re-imagine the vignette through the lens of prosocial behaviors. The day would start with verbal recognition of the pressures the team members are feeling to help improve engagement in the team effort. In addition, pre-planning as a team can help reduce the impact of production pressure and allow each team member to exert some influence on how the day will run.
The big picture here is that by defining these core design principles for effective group collaboration, there is a validated scientific foundation for prosocial change. Acceptance and Commitment Training or ACT can help develop positive change for individuals, groups, and organizations. This training is a validated methodology for managing burnout and negative behaviours while maintaining healthy and cooperative working environments. The authors provide the ACT Matrix which is an analytical tool for applying ACT training to individual and group behaviors by analysing the environment and understanding behaviors that move away or towards desired goals. Check out Figure 1 in the article. Individuals must learn how to notice when their behaviors are counterproductive and develop psychological flexibility to adopt productive behaviours.
The matrix takes you from the current state to a future desired state. In the middle are specific behaviors that move the individual or group towards the future state which is labelled engaging or helping move towards success or move away which is labelled as avoiding or obstructing you from success. The vertical access indicates the differences between outer actions or public behavior and inner thoughts and feelings or private behavior and what we experience. In the centre of the matrix is Noticing since individuals must notice these behaviors and develop the ability to replace avoiding behaviors with engaging behaviors.
You can check out the matrix in the article and I will include it in the show notes. We can apply the matrix to the vignette. For example, in the current state, production pressure is endemic due to economic incentives and fosters behaviours that impeded team performance. The inner thoughts and feelings on the avoiding side of the matrix include the following:
For the surgeon, team members insensitive to the work required to bring patients to the facility.
For the anesthetic team, requirements for safe anesthesia care are not viewed as consistent with efficiency. Staffing not consistent with patient care demands.
And for nursing, targets for OR efficiency lead to expectations for work and overtime that are inconsistent with available staff.
If we move right in the matrix, the engaging behaviours for all may include:
Each member of the group has a mindset to help each other in their respective jobs throughout the day. Personal connection between members of the team providing patient care is valued.
Then, the future desired state may include a work environment that fosters interpersonal connection leading to staff retention and easy recruitment. Each team member understands that supporting the work of each member will lead to a safer, more efficient experience. Advance preparation and communication between team members ensures that there is adequate time to complete the scheduled patient care and equipment and supplies are available. At the conclusion of each procedure, the team discusses any obstacles that arose to safe and efficient care including equipment and individual behaviors. Management support is readily available to help address barriers to care. Efficiency and wellbeing metrics are tracked with feedback to the group and invitation for suggestions to make improvements as needed.
I don’t know about you, but that future desired state sounds like a pretty good place to work.
So, how do we change the culture in the operating room environment? We need to recognize the limitations of the existing culture and the potential value for making the change. Perhaps, the current staffing shortages leading to burnout syndrome in healthcare can be a motivating factor. Plus, with increasing efficiency goals, prosocial behaviors and team work can bring groups of people together to help meet these goals. The authors tells us that the potential value of prosocial change is to create a culture that fosters highly functional teams that maximize efficiency and derive job satisfaction from collegial relationships and collectively achieving shared goals. It is easy to see why this is a desirable goal, but the path to success in procedural areas in healthcare is not defined and new methods are needed.
Let’s see what happens if we inject some prosocial behaviors into the clinical vignette that we read last week. Okay, once again we have an 8-hour block where 3 cases have been scheduled including 2 robotic prostatectomies and a cystoscopy. Here we go:
“The day prior to the OR day, all professionals to be involved with the cases are scheduled and notified. The surgeon sends a group text acknowledging that the schedule is ambitious and indicates that she will be available at the start of the day to help the team manage the day. Nursing leadership ensures that the circulator and scrub tech have an opportunity to discuss the setup for the next day in advance. The anesthesia team reviews the patient together and plans to manage a fiberoptic-guided intubation. The anesthesiologist communicates with the team in his other room with the goal of minimizing any delay to the start of the robotic cases.
On the morning of the procedure, the team huddles 20 minutes prior to the anticipated start of the case. At that point, the patient has been evaluated in the preop area by both the surgeon and anesthesiologist. The circulator is instructing the new scrub tech on preparing a robotic procedure, reinforcing the discussion from the prior day. The nurse anesthetist brings the patient into the room on time, is well-prepared for induction and intubation after the prior discussion with the anesthesiologist, and can begin monitoring and sedating the patient. The anesthesiologist joins 10 minutes later after starting the other room. During the process of induction and fiberoptic intubation, the surgeon (who has remained in the room) offers to assist the anesthesia team so the circulator and scrub tech can continue to prepare equipment for the procedure.
As the timeout checklist begins, the surgeon states, “Let’s take a moment to ensure we are all set for the day. If anyone has any concerns or needs support, now is the time to speak up.” The circulating nurse introduces the scrub tech who is in training by name, and the anesthesiologist introduces the visiting nurse anesthetist. These new team members are welcomed and encouraged to ask any questions. The anesthesiologist indicates he is covering two rooms and identifies the need for communication to coordinate the work in both rooms throughout the day.
Towards the end of the second case, the procedure time is running longer than expected, and the surgeon invites the team to discuss any challenges to starting the last case and completing the day on time. The circulator states that he can stay for a short time after the scheduled day to take care of the patient, but the surgeon encourages them to speak to nursing leadership before starting the case to ensure there is relief if needed. The team works quickly to turn over the operating room and begin the last case. Despite their efforts, the last case runs 30 minutes late, but everyone wants to finish the day together. As the anesthesia team exits the room with the patient, everyone expresses appreciation for the communication and teamwork during the day.”
This revised scenario involves prosocial behaviors where all team members act in ways that demonstrate mutual respect and support in the service of safe and effective patient care. We can measure team efficiency, staff wellness, and retention and use these measures to assess the impact of prosocial behaviors. There is a call to action to look at our existing culture and evaluate the potential impact of prosocial culture change on team engagement and performance including safe perioperative care.
Before we wrap up for today, we are going to hear from one of the authors. Here she is now.
[Mary] “ Hi, my name is Mary Faron. I’m a member of the Association of Perioperative Registered Nurses and a circulating RN working at Swedish Medical Center in Seattle, Washington. AORN is excited to partner with our anesthesia colleagues at APSF in exploring options at perioperative team performance. We believe the interdisciplinary approach is important for the success of any culture change in this complex arena of perioperative teams.
AORN has posted a link to this article on the website for member access. There will also be a guest editorial in the May edition of the AORN Journal, highlighting this publication of the white paper in the APSF newsletter. I hope that you’ll share this paper with your perioperative team.”
Thank you so much to the authors for contributing to the show and for your hard work on this project. For more information about prosocial behaviors, head over to prosocial.world. I will include a link in the show notes as well.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
We hope that you will subscribe so you don’t miss an epsiode, share this with a colleague who’s feeling the pressure, and leave a review to help more clinicians find the show.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2026, The Anesthesia Patient Safety Foundation
