Episode #287 A New Era For PONV: Safety, Guidelines, And Smarter Rescue
December 31, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
As 2025 draws to a close, we are returning to 2 of our most popular episodes to bring you a special revisited show today. We are returning to Episodes #141 and #142. Our featured article is from the February 2023 APSF Newsletter. It is “Dopamine-Antagonist Antiemetics in PONV Management: Entering a New Era?” by Connie Chung and Joseph Szokol.
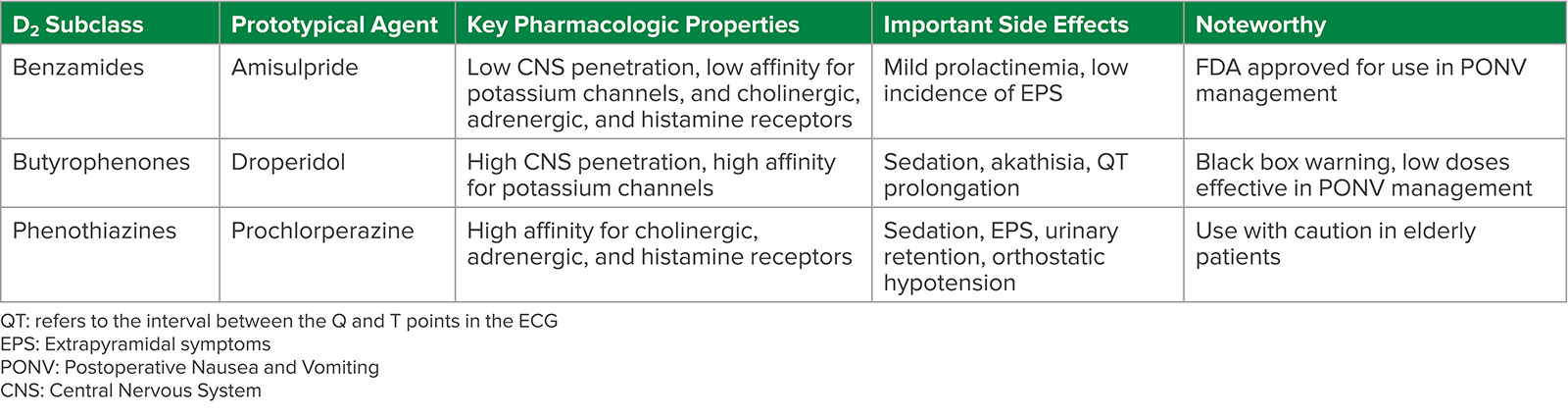
Table 1: D2 Subclass of Antiemetics
Here is the citation for the 2020 Cochrane network meta-analysis that we talked about on the show today:
Weibel S, Rucker G, Eberhart LH, et. al. Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis. Cochrane Database Syst Rev.2020;10:CD012859. PMID: 33170514.
The authors highlight two important considerations from the Fourth consensus guidelines published in 2020.
- Prevention of PONV must be a critical component of anesthesia care. Patients with even just one or two risks factors for PONV should receive multimodal PONV prophylaxis.
- PONV treatment should include the use of an antiemetic medication from a different pharmacologic class than the initial prophylactic medication.
Here are the citations to the additional articles that we talked about on the show today.
Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg.2020;131:411–448. PMID: 32467512.
Kranke P, Bergese SD, Minkowitz HS, et al. Amisulpride prevents postoperative nausea and vomiting in patients at high risk: a randomized, double-blind, placebo-controlled trial. 2018;128:1099–1106. PMID: 29543631.
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We are returning to two of our most popular episodes of all time to bring you a special revisited show today. Our conversation covers one of the most important topics for anesthesia professionals and our patients. This is a topic that may come up during a preoperative interview, something that may alter our anesthesia plan intraoperatively, and is a postoperative complication that may delay discharge from the PACU. So, stay tuned.
Before we dive into the episode today, we’d like to recognize GE Healthcare, a major corporate supporter of APSF. GE Healthcare has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, GE Healthcare – we wouldn’t be able to do all that we do without you!”
Have you figured out what we are talking about today? That’s right, it is postoperative nausea and vomiting. Our featured article today is “Dopamine-Antagonist Antiemetics in PONV Management: Entering a New Era?” by Connie Chung and Joseph Szokol from the February 2023 APSF Newsletter. To follow along with us, head over to APSF.org and click on the Newsletter heading. The fourth one down is Newsletter archives. From here, scroll down to the February 2023 Newsletter and our featured article today. I will include a link in the show notes as well.
And now, let’s return to episodes # 141 and #142 all about Postoperative Nausea and Vomiting Management. Here we go…
[Insert Episode #141] Before we get into the article, we are going to hear from one of the authors, Connie Chung. Let’s take a listen.
[Chung] “Hi, my name is Connie Chung, and I’m an anesthesiologist at the University of Southern California Keck School of Medicine in Los Angeles, California. I’m also the medical director of our outpatient surgery center.”
[Bechtel] To kick off the show today, I asked her why she wrote this article.
[Chung] “Postoperative Nausea and Vomiting, or PONV for short is a topic I’m very passionate about. We want all of our patients to have a great perioperative experience, and PONV can really leave a bad taste in your mouth. All jokes aside, PONV also contributes to prolonged recovery room stays, unanticipated hospital admissions, and increased healthcare costs. Moreover, as a non-smoking female who experiences motion sickness, I know that I personally am in the highest risk category for PONV. It is exciting to see that there is now an FDA approved agent that can be used as rescue treatment of PONV after failed prophylaxis.”
[Bechtel] It is really excited to see a new medication that can be used for treatment of PONV. Before we head into the new era for PONV treatment, let’s review where we have been. The authors remind us that Dopamine D2-receptor antagonists were the primary treatment for post-operative nausea and vomiting for the second half of the last century. Then, at the start of the 21st century, the use of these medications decreased due to safety concerns as well as the publication of a black box warning by the US Food and Drug Administration on Droperidol which was the most commonly used Dopamine D2-receptor antagonists. Have you used Droperidol for the management of PONV in your practice? Did your practice change after the black box warning?
There is a new kid on the block for the treatment of PONV. In 2020, the FDA approved Amisulpride for the prevention and treatment of PONV and it is the only approved agent for rescue treatment after failed prophylaxis.
One of the things we have learned about D2-antagonists is that even drugs that are in this same drug class have different safety and efficacy profiles. There are at least three distinct structural sub-classes with a different pharmacologic properties and side effects. The sub-classes include:
- Substituted Benzamides
- Butyrophenones
- Phenothiazines
Check out Table1 in the article. It includes the subclasses, the prototypical agent, key pharmacologic properties, important side effects, and noteworthy considerations. We are going to review it now.
First up is the Benzamides group. Amisulpride belongs to this subclass. Key properties include the following: Low CNS penetration as well as low affinity for potassium channels and cholinergic, adrenergic, and histamine receptors. The important side effects include mild prolactinemia and low incidence of Extrapyramidal symptoms. Finally, Benzamides are FDA approved for use in PONNV management.
Next up is the Butyrophenones which includes Droperidol. Droperidol has high CNS penetration and a high affinity for potassium channels. Side effects include sedation, akathisia, and QT prolongation. Key considerations include black box warning and low doses are effective in PONV management.
The third subclass is Phenothiazines. Prochlorperazine belongs to this class. Key properties include high affinity for cholinergic, adrenergic, and histamine receptors. Side effects include sedation, extrapyramidal symptoms, urinary retention, and orthostatic hypotension. Administration of this drug to elderly patients may not be appropriate due to these side effects and safety concerns.
Speaking of safety, the authors highlight the safety profile of D2-antagonists. The early D2-antagonists included neuroleptics and first-generation antipsychotics. There was a wide range of neurological effects ranging from sedation to neuropsychiatric including dysphoria or cognitive impairment, due to central nervous system penetration. Another considerable side effects included extrapyramidal symptoms such as tardive dyskinesia, dystonia, and akathisia which limited use. Don’t forget about the risk of neuroleptic malignant syndrome or NMS. Patients may present with fever, mental status changes, muscle rigidity, autonomic instability, and hyperprolactinemia from blockade of D2-receptors in the pituitary gland. There are cardiac side effects as well since binding to potassium ion channels may lead to QT prolongation and torsade de pointes.
The newest medication, Amisulpride, is considered to be atypical or a second-generation antipsychotic with decreased CNS penetration and decreased adverse effects. It is important to keep in mind that some of the side effects from d2-antagonists are dose-dependent, but just decreasing the dose may not be the answer since there is limited data about dose reduction and efficacy. There may be a significant impact on patient safety due to the adverse reactions such as tardive dyskinesia, dysphoria, and torsade de pointes.
Let’s move on to talk about the different classes of medications and we are going to start with Benzamides. Remember, this is the drug class that Amisulpride is in. Amisulpride is a substituted benzamide D2-antagonist and 5-HT2B and 5-HT7A serotonin antagonist with low blood-brain barrier penetration and decreased affinity for adrenergic histamine and cholinergic receptors leading to less anticholinergic and sedative effects. There is also a lower incidence of extrapyramidal symptoms since Amisulpride has preferential binding in the limbic system. There is even more good news in the literature.
A 2020 Cochrane network meta-analysis revealed that Amisulpride has a similar incidence of adverse events when compared to placebo. The risk for adverse effects following administration is lower: Prolactin levels are not elevated above the normal levels for nonpregnant women. Amisulpride also has a weaker affinity for potassium channels and thus does not prolong QT intervals when used at PONV management doses. Finally, amisulpride is effective for preventing PONV as well as for rescue treatment.
Metoclopramide is another medication in this drug sub-class. It is a weak D2 and 5-HT3 antagonist with dose dependent side effects including sedation, extrapyramidal symptoms, and GI upset due to stimulation of gastric smooth muscle cells. Metoclopramide is not as effective for treatment of PONV, but may be considered if there is limited access to other D2-antagonists.
Our next drug class is the Butyrophenones. Droperidol is in this class and historically was administered in low doses for first-line treatment for PONV. Side effects include sedation, dysphoria, anxiety, akathisia, and QT prolongation. You are probably already aware of the risks of QT prolongation since the FDA applied a black box warning in 2001 due to this risk leading to sudden cardiac death. After the black box warning, Droperidol administration for PONV prophylaxis declined significantly. Recently, a new study, the 2020 Cochrane network meta-analysis revealed that antiemetic doses of Droperidol had a similar incidence of adverse events compared to placebo. The most common doses for Droperidol in this study included 0.625-1.25mg IV given at induction of anesthesia. After the FDA black box warning was placed on Droperidol, the focus shifted to Haloperidol, another butyrophenone medication that may be used for treatment of PONV. Adverse side effects included sedation, extrapyramidal symptoms, neurotoxicity, and QT prolongation. In 2007, the FDA updated the labeling for Haloperidol to remind clinicians that this medication is not approved for IV administration for PONV treatment and its use in high doses is associated with torsade’s de pointes and QT prolongation. Keep in mind that a single, low dose of IV Haloperidol may be used for PONV prophylaxis and is likely safe and effective.
The third subclass is Phenothiazines. Prochlorperazine is the most common medication I this class for PONV management. Adverse effects include the following:
- Sedation
- Extrapyramidal symptoms
- Anticholinergic effects such as anorexia, blurred vision, constipation, dry mucosa, and urinary retention
- Antiadrenergic effects leading to orthostatic hypotension
- Decreased seizure threshold.
Another phenothiazine D2-antagonist is promethazine which also has antihistamine effects and may produce sedation. Caution must be used with IV administration since severe tissue damage may occur following extravasation from a vein.
Now that we have reviewed the different subclasses, less talk about side effects from D2 antagonists. Remember, the D2-antagonists are not recommended to be used for patients with prolonged QT syndrome or in combination with other medications that prolong the QT interval. The FDA black box warning on Droperidol highlighted the risk for QT prolongation, but the authors remind us that Ondansetron, which does not have a black box warning and is a commonly used antiemetic medication, can also prolong the QT interval, but the QT prolongation from the combination of ondansetron and Droperidol is not longer than that induced by either drug alone.
There are several home medications that may lead to significant adverse effects when D2-antagonists are administered during the perioperative period.
- Be on the lookout for QT prolongation when D2-antagonists are administered for patients taking medications that either reduce the HR or induce hypokalemia.
- Patients taking antipsychotic medications are at risk for tardive dyskinesia and NMS.
- Do not administer D2-antagonists to patients taking dopamine agonists including Levodopa for Parkinson’s or Cabergoline for hyperprolactinemia.
- It is also important to avoid co-administration with monoamine oxidase inhibitors since norepinephrine is broken down by MAO and the D2-blockade leads to build-up of norepinephrine and an exaggerated end-organ response.
One of the APSF Priorities is Perioperative Brain Health which includes perioperative delirium, cognitive dysfunction, and brain health. This is an important consideration with the use of D2 antagonists. The authors advise caution with or avoidance of administration of D2-antagonist for PONV management in patients older than 65 years old due to the risks of central anticholinergic effects (this is the phenothiazine subclass), extrapyramidal symptoms (from the benzamides) and tardive dyskinesia, delirium, and NMS from the butyrophenones. There is an increased risk for cerebrovascular accident, cognitive dysfunction, and mortality in elderly patients who receive these medications. But you must also remain vigilant in pediatric patients who may develop extrapyramidal symptoms or QT prolongation following administration of D2 antagonists.
[New Clip Bechtel] There is still more to talk about related to D2-antagnoists and PONV management so we are going to continue on with Episode #142. We promised you a supersized episode today so let’s keep the conversation going as we discuss PONV clinical practice guidelines.
[Insert Episode #142]
“Let’s take a step back from the treatment of PONV to talk about PONV in general. Postoperative nausea and vomiting or PONV is an important consideration for anesthesia patient safety that may have a big impact on prolonged post anesthesia care unit length of stay, unanticipated hospital administration, and increased health care costs. Recently, in 2020, the fourth consensus guidelines for the management of POMV was published which outlines identification of high-risk patients, managing baseline PONV risks, choices for prophylaxis, and rescue treatments for PONV. The authors highlight two important considerations from the guidelines:
First, prevention of PONV must be a critical component of anesthesia care and patients with even just one or two risks factors for PONV should receive multimodal PONV prophylaxis.
Let’s take a quick commercial break to review the risk factors for PONV from the fourth consensus guidelines which include the following:
- Female sex
- History of PONV or motion sickness
- Nonsmoking
- Younger Age
- General versus Regional Anesthesia
- Use of Volatile Anesthetics and Nitrous Oxide
- Postoperative opioids
- Duration of anesthesia
- And type of surgery including cholecystectomy, laparoscopic, and gynecological procedures.
There is conflicting evidence for the following factors and the impact on PONV:
- ASA physical status
- Menstrual cycle
- Level of anesthesiologist’s experience
- And Perioperative fasting.
Here are some factors that have been either disproven or shown to be of little clinical relevance:
- BMI
- Anxiety
- Presence of a nasogastric tube
- History of migraines
- And Use of supplemental oxygen.
And now, back to the APSF article for the 2nd point highlighted by the authors.
PONV treatment should include the use of an antiemetic medication from a different pharmacologic class than the initial prophylactic medication. That’s right, there is no benefit of re-dosing ondansetron even though this is a common practice.
Before we get to the exciting conclusion of the APSF article, let’s review the fourth consensus guidelines. I will include the citation in the show notes as well. Table 3 provides a plan to decrease the baseline risk for PONV which involves the following steps:
- Avoidance of GA by using regional anesthesia
- Use of propofol for induction and maintenance of anesthesia
- Avoidance of nitrous oxide in surgeries that are longer than 1 hour
- Avoidance of the use of volatile anesthetics
- Multimodal analgesia with a goal to minimize intraoperative and postoperative opioid administration
- Providing adequate hydration
- Use of Sugammadex rather than neostigmine for reversal of neuromuscular blockade.
Table 4 in the consensus statement provides a list of antiemetic medications with the dose and timing for adults. We are going to review a few of these.
- Amisulpride 5mg given at induction
- Dexamethasone 4-8mg IV given at induction
- Droperidol 0.625mg IV given at the end of surgery
- Haloperidol 0.5- less than 2mg IM or IV
- Metoclopramide 10mg
- Ondansetron 4mg IV given at the end of surgery
- Promethazine 6.25mg
- And Scopolamine transdermal patch given the evening prior or 2 hours preop
There is so much great information in the fourth consensus guidelines, let’s take a look at one more graphic. Figure 6 is an infographic that displays an algorithm for PONV management in adults. Step 1 is identifying risk factors. Step 2 is risk mitigation using some of the steps that we outlined earlier. Step 3 includes risk stratification and patients with 1-2 risk factors should receive 2 agents and patients with more than 2 risk factors should receive 3-4 agents. Step 4 is prophylaxis options, and step 5 involves rescue treatment using an antiemetic from a different drug class than the prophylactic class. As we work through the algorithm for the management of PONV in adults it is important to remember that the combination of non D2-antagonist antiemetic medications combined with older D2 antagonists like Droperidol, haloperidol, and promethazine are more effective than either agent alone. More recently, amisulpride has been evaluated in 6 clinical trials. In 5 of these trials, amisulpride was studied as the sole antiemetic drug and found to be superior to placebo for prevention and treatment of PONV. The 2018 study in Anesthesiology, “Amisulpride prevents postoperative nausea and vomiting in patients at high risk: a randomized, double-blind, placebo-controlled trial” reported that the combination of amisulpride with ondansetron or dexamethasone was more effective than ondansetron or dexamethasone along for preventing PONV or for rescue treatment. I will include this citation in the show notes as well.
Management of PONV is multifactorial including prevention as well as management and this is a vital component of the anesthetic plan especially as part of the enhanced recovery after surgery pathways, for patients undergoing ambulatory surgery, and for high risk patients with high acuity and fragility levels. As we have talked about for the past two episodes D2-antagonists are effective medications for PONV management, but understanding the side effects, effective doses, and route of administration is critical. The future of PONV management is bright with a new option, Amisulpride, which is a D2 antagonists with less side effects and excellent efficacy for prevention and rescue treatment.
Before we wrap up for today, we are going to hear from one of the authors of the APSF Newsletter article, Connie Chung again. I asked her, “What do you hope to see going forward?” Let’s take a listen to what she had to say.
[Chung] “I really take to heart what is stated in the fourth consensus guidelines for the management of PONV published in anesthesia and analgesia in 2020. The prevention of PONV should be considered an integral aspect of anesthesia. However, sometimes despite our best efforts to identify high risk patients and administer prophylaxis, patients still develop PONV, and now there’s an FDA-approved treatment option for PONV with a favorable safety profile. My hope is that more patients can benefit from the use of Amisulpride.”
[Bechtel] Thank you so much for Chung for contributing to the show today. We hope more patients can benefit from treatment with Amisulpride when it comes to managing PONV going forward. We will be on the look out for future studies and a cost-benefit analysis related to this newer medication. Do you have Amisulpride at your institution? Have you used it for PONV management? Let us know by tagging up on twitter @APSForg using the hashtag, #apsfpodcast.
We made it to the end of the article, but we also need to address a threat to anesthesia patient safety for our pediatric patients. That’s right the management of PONV in children is so important. If we look at the fourth consensus statement, there are several considerations. First, reducing baseline PONV risk may include the use of TIVA, liberal fluid therapy, and opioid-sparing techniques. There is some evidence that IV lidocaine, IV acetaminophen, and alpha-2 agonists as part of a multi-modal anesthetic plan may help to decrease rates of PONV. PONV prophylaxis in children may include administration of the following medications:
- Aprepitant 3mg/kg up to 125mg
- Dexamethasone 150mcg/kg up to 5 mg
- Droperidol 10-15 mcg/kg up to 1.25mg
- And Ondansetron 50-100mcg/kg up to 4 mg
Looking a little closer at the fourth consensus guidelines, the authors report that when the risk for PONV is very low and the surgery is less than 30 minutes long, PONV prophylaxis may not need to be administered. For longer surgeries or patients at high risk, prophylaxis with a combination of medications is recommended. What is your preferred PONV prophylaxis combo for pediatric patients? The strongest evidence supports administration of dexamethasone plus ondansetron for prophylaxis.”
[Bechtel] Thank you for joining us for this end of year revisited special episode edition. We’ll be back in the New Year with all new episodes as we continue to work towards improved anesthesia patient safety.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
