Episode #269 Infiltrated IV Crisis: Managing Complications and Keeping Patients Safe
August 27, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is from the June 2025 APSF Newsletter. It is “Treatment and Complications of IV Infiltration of Neuromuscular Blocking Agents” by Govind Rangrass, MD, FASA; Karolina Brook, MD, FASA, CPPS; Rachel C. Wolfe, PharmD, MHA, BCCCP, FCCP; Fenghua Li, MD, FASA; Andrea Vannucci, MD, FASA, CPPS.
Thank you so much to Govind Rangrass, Karolina Brook, and Andrea Vannucci for contributing clips to this podcast series.
Here is the authors’ proposed algorithm to manage the complication of IV infiltration of neuromuscular blocking drugs:
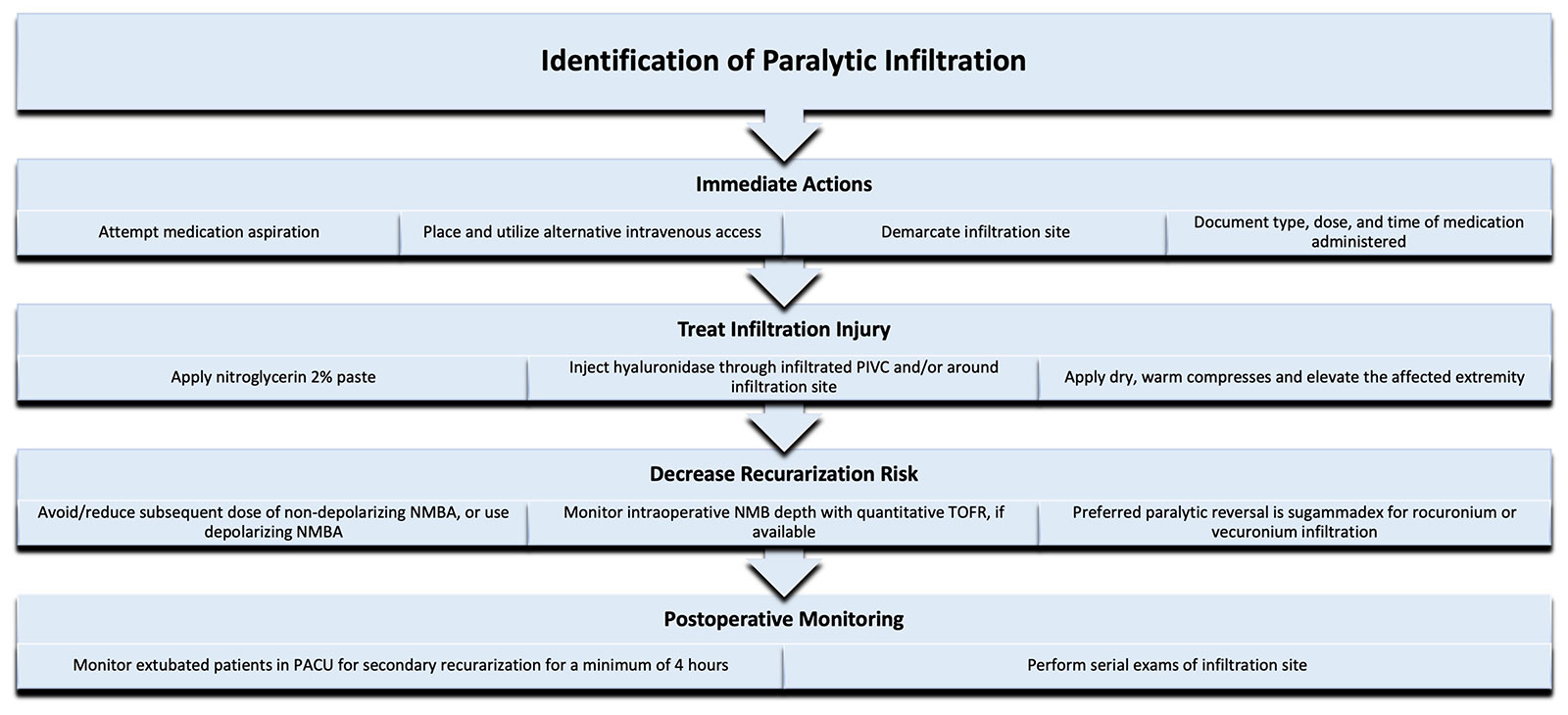
Figure 1: Authors’ proposed algorithm to manage paralytic extravasation.
Neuromuscular blocking agent (NMBA); Neuromuscular blockade (NMB); Post-anesthesia care unit (PACU); Train-of-four ratio (TOFR).
The 2025 APSF Stoelting Conference is right around the corner on September 3rd-4th. The focus for this years conference is “Transforming Maternal Care: Innovations and Collaborations to Reduce Morbidity and Mortality.” Conference objectives include innovative strategies to reduce severe maternal morbidity, actions that anaesthesia clinicians can take to advance birth equity, the role of anesthesia professionals to reduce preventable causes of maternal mortality, and identify opportunities for collaboration across role groups to overcome current maternal care challenges. This is a high-yield conference for anyone interested in keep patients safe during maternal anesthesia care. You can register for the livestream. Plus, we will be featuring highlights from the conference on upcoming podcast episodes so you don’t miss a thing.
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We are back for part 2 of our series all about how to keep patients safe following IV infiltration of neuromuscular blocking agents. Plus, we have more exclusive content from one of the authors.
Before we dive further into the episode today, we’d like to recognize Merck, a major corporate supporter of APSF. Merck has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Merck – we wouldn’t be able to do all that we do without you!”
Our featured article once again today is “Treatment and Complications of IV Infiltration of Neuromuscular Blocking Agents” Rangrass and colleagues. To follow along with us, head over to APSF.org and click on the Newsletter heading. The first one down is the current newsletter. Then, scroll down until you get to our featured article today. I will include the link in the show notes as well.
Have you placed any peripheral intravenous catheters this week? Did any of these infiltrate? Peripheral IV cannulation is the most common invasive procedure performed in hospitals. Anesthesia professionals need to stay vigilant for complications which may include nerve injury, vascular injury, and infiltration. IV infiltration is the unintended administration of any medications or fluids into tissues surrounding the catheter and occurs in about 14% of peripheral IV catheter insertions. We talked about this threat to anesthesia patient safety last week on the show and we are going to continue the conversation today.
To help kick off the show today, we are going to hear from one of the authors. I will let him introduce himself now.
[Govind Rangrass] “ Hello, my name is Govind Rangrass, and I’m a professor of anesthesiology and critical care at SSM Health St. Louis University Hospital, where I also serve as the Director of Patient Safety and Quality.”
[Bechtel] I asked Rangrass why he wrote this article? Let’s take a listen to what he had to say.
[Rangrass] We wrote this article because IV infiltration is a surprisingly common complication in perioperative care, but there is very little guidance on how to manage it, especially when it involves the infiltration of neuromuscular blocking agents. We believe that stakes are high. If a paralytic is administered into compromised IV access, it can lead to delayed or even failed induction and complicate safe emergence from anesthesia. Our goal by writing this article was to highlight this overlooked issue and offer an algorithmic approach that anesthesiologists can use immediately.
We also hope that it serves as a call to action for further research and consensus building within the field. Why do you feel so passionate about this topic or area? Uh, I personally am passionate about this topic because it combines a very practical clinical challenge with patient safety implications that are often under recognized.
IV infiltration is something that we’ve all seen, but when a paralytic is involved, the complexity skyrockets and there’s almost no literature to guide us. It’s really deeply unsatisfying from a clinical and academic standpoint to tell a colleague. There’s no clear answer here, and I think our colleagues deserve better and so do our patients.
So that’s really what primarily drove us to dive deeper and help create something actionable for the anesthesia community.
[Bechtel] Thank you so much to Rangrass for helping to kick off the show today. It’s time to talk about the management of neuromuscular blocking agent infiltration. Here we go.
Oh no, the peripheral IV catheter infiltrated on induction of anesthesia. The first step is to leave the infiltrated catheter in place and attempt to aspirate medication. Next, review the medications that were administered into the infiltrated catheter. If a non-depolarizing neuromuscular blocking agent was used, then once you have a new peripheral IV catheter, it is important to consider using a reduced dose of any further non-depolarizing neuromuscular blocker or avoid any redosing of a non-depolarizing neuromuscular blocking agent or change to succinylcholine. During the surgery, there are a few steps that you can take to help keep patients safe as well including the following:
Elevate the extremity with the infiltration
Apply a warm compress with dry heat to aid in systemic uptake of the drugs
Demarcate the area of the infiltration
Consider administration of hyaluronidase through the infiltrated catheter and intradermally around the leading edge of the infiltration site.
Conduct serial exams of the area and consult surgery if there are concerns for tissue injury or compartment syndrome.
Check out Figure 1 in the article for the authors proposed algorithm to help manage paralytic medication infiltration. You can use this as an important resource to manage this event and help prevent harm from this complication. I will include the figure in the show notes as well.
Now, let’s talk about some of these steps in a little more detail. The onset and duration of action of infiltrated rocuronium depends on local circulation and systemic absorption. Improving the systemic absorption of the infiltrated rocuronium enables reversal in the immediate intraoperative period. There are two medications that have been used to help increase systemic absorption of many infiltrated medications: Hyaluronidase and Nitroglycerine paste.
Hyaluronidase is an enzyme that hydrolyzes hyaluronic acid to help with the absorption and dispersal of injected medications. It is often used to treat severe infiltration events with pH-related and hyperosmolar vesicants. Hyaluronidase comes in a 1mL vial with 150 units and should be administered with tuberculin syringe and 25g or smaller needle. Time is of the essence since administration of this medication should occur within 1 hour of the infiltration event and you may begin to see improvements in swelling within 15-30min of enzyme delivery along the tissue plane. Here are the steps for one of the recommended administration methods:
- Dilute hyaluronidase to 15 units/mL
- Perform five 0.2mL injections for a total of 1mL around the leading edge of the infiltration site.
- Prior to removal of the infiltrated catheter, 15 units may be administered through the catheter and repeated every 30-60 minutes until the infiltration site resolves
Another option is to take advantage of the vasodilating effects of nitroglycerin 2% paste to improve systemic drug absorption. You can apply this to one square inch areas of infiltration, but you will need to avoid any areas of skin breakdown.
Once you get to the end of the surgery, it is time for neuromuscular blockade reversal. There is not a lot in the literature to guide us since there are only 12 case reports and one prospective study that addresses the pharmacokinetics and pharmacodynamics of subcutaneously administered steroidal neuromuscular blocking agents. Looking at the case reports, there were only about 30 patients and the medications used were pancuronium, vecuronium, and rocuronium. There are no infiltration reports from cases where benzykusiquinoline alkaloids were used and this may be due to their spontaneous degradation at tissue pH helps to protect against complications related to resorption. For reversal following an infiltration event, it is important to consider monitoring the depth of blockade as well as the patient’s hepatic and renal function.
Sugammadex is the preferred agent for reversal of rocuronium and vecuronium. Here are several options depending on resource availability.
For patients who continue to have deep levels of blockade or if sugammadex is not available, they may need to remain intubated postoperatively until intact neuromuscular function as been restored.
If only qualitative monitoring is available or there is concern for residual neuromuscular blocking agent at the infiltration site and the depth of blockade is mild to moderate, administer standard reversal doses and monitoring the patient for recurarization in the PACU.
If quantitative train of four ratio monitoring is used and the infiltration site has visibly improved, reversal can be guided by the train of four ratio data and patients can be monitored clinically for residual paralysis. Consider reducing the stimulation current to below 40 milliamperes using a electromyography-based quantitative train of four ratio monitor if needed in the PACU.
Once extubated, patients without hepatic and renal dysfunction should be monitored in the PACU for at least 4 hours and the patient and nursing teams will need to be informed about the signs and symptoms of residual blockade with a plan to guide escalation of care.
The authors leave us with a call to action for anesthesia professionals to remain vigilant for infiltration events and be prepared to manage patient injuries and prevent secondary recurarization when neuromuscular blocking agents are involved to help keep patients safe from harm following this complication.
[Bechtel] Before we wrap up for today, we are going to hear from Rangrass again. I also asked him what do you envision for the future with regards to this area of anesthesia care? Here is his response. Looking ahead. I envision a future where we have standardized guidelines for managing IV infiltration in the or, especially when paralytics are involved.
Ideally, this will be a topic that’s integrated into residency training and crisis checklists, just like anaphylaxis or local anesthetic, systemic toxicity. I’d also love to see greater integration of safety technologies that can detect. Infiltration early, but most of all, I just hope that our work sparks further discussion, data collection, and consensus building so that our, uh, very, this very real clinical problem is no longer treated as a footnote.
[Bechtel] Thank you so much to Rangrass for contributing to the show today. We are looking forward to a future with readily available checklists for managing IV infiltration and tools to help detect and even prevent this complication going forward.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
The 2025 APSF Stoelting Conference is right around the corner on September 3rd-4th. The focus for this years conference is “Transforming Maternal Care: Innovations and Collaborations to Reduce Morbidity and Mortality.” Conference objectives include innovative strategies to reduce severe maternal morbidity, actions that anaesthesia clinicians can take to advance birth equity, the role of anesthesia professionals to reduce preventable causes of maternal mortality, and identify opportunities for collaboration across role groups to overcome current maternal care challenges. This is a high-yield conference for anyone interested in keep patients safe during maternal anesthesia care. You can register for the livestream. Check out the conference link in the show notes for more information. Plus, we will be featuring highlights from the conference on upcoming podcast episodes so you don’t miss a thing.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
