Episode #257 Sweet Trouble: Perioperative Management of SGLT2 Inhibitors
June 4, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
We are returning to the February 2025 APSF Newsletter today. Our featured article is “Editorial: Euglycemic Ketoacidosis Concerns in Perioperative Use of SGLT2 Inhibitors: Re-Examining Current Recommendations” by Soyun M. Hwang, MD; Arney S. Abcejo, MD; Adam K Jacob, MD; Jesse M. Raiten, MD; and Manpreet S. Mundi, MD.
Check out Figure 1 in the article for recommendations for perioperative management of SGLT2 Inhibitors. Do you have a protocol that you follow at your institution for patients taking SGLT2 inhibitors? If not, you may consider using this algorithm. This is an important way that anaesthesia professionals can help to keep patients taking SGLT2 inhibitors safe during and after anaesthesia care.
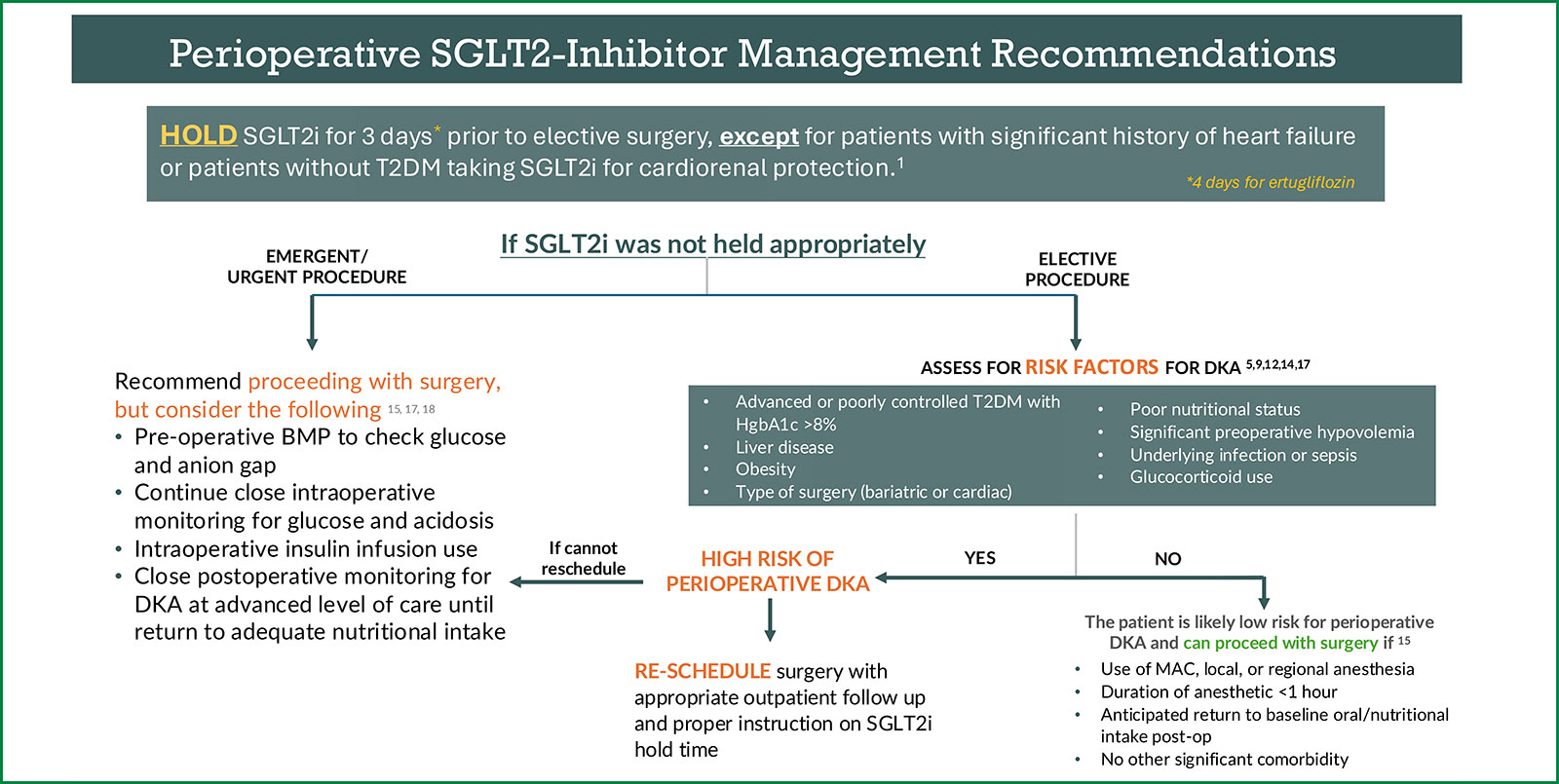
Figure 1: Recommendations for perioperative management of SGLT2i. Management pathways are influenced by the urgency of surgery and other significant patient or surgical factors that may increase risk of perioperative diabetic ketoacidosis. This algorithm does not apply to nondiabetic patients taking SGLT2i for heart failure or cardiorenal protection, as data suggest they should continue SGLT2i. Note that there are no Class 1 evidence for the perioperative management of SGLT2i. SGLT2i: Sodium-Glucose Cotransporter-2 Inhibitor; BMP: Basic Metabolic Panel; T2DM: Type 2 Diabetes Mellitus; DKA: Diabetic Ketoacidosis; MAC: Monitored Anesthesia Care.
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. It is almost time for the release of the June 2025 APSF Newsletter, but there is still time for us to return to the February 2025 Newsletter. We are checking out the Editorial article today. Sodium-glucose co-transporter-2 inhibitors or SGLT2 inhibitors are used for treatment of type 2 diabetes mellitus. There are additional benefits for these medications for patients with heart failure and chronic kidney disease as demonstrated by the EMPEROR and CANVAS randomized controlled trials. This means that patients taking SGLT2 inhibitors are coming to an operating theatre near you and you need to be prepared to provide safe anesthesia care.
Before we dive further into the episode today, we’d like to recognize Merck, a major corporate supporter of APSF. Merck has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Merck – we wouldn’t be able to do all that we do without you!”
We are returning to the February 2025 APSF Newsletter today. Our featured article is the Editorial, “Euglycemic Ketoacidosis Concerns in Perioperative Use of SGLT2 Inhibitors: Re-Examining Current Recommendations” by Hwang and colleagues. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the Current Issue. Then, scroll down until you get to our featured article today. I will include the link in the show notes as well.
This is an important topic for anesthesia professionals since there are concerns about patients developing euglycemic ketoacidosis which is an uncommon but life-threatening side effect associated with SGLT2 inhibitor use. SGLT2 inhibitor medications inhibit glucose reabsorption in the proximal convoluted tubule leading to glycosuria and reductions in serum glucose levels without an increase in insulin levels. Glucagon production may also be increased leading to lipolysis, ketoacid production, and rarely anion gap metabolic acidosis. There is an increased risk during the perioperative time period due to fasting and increased stress hormones, so anesthesia professionals need to be aware and prepared.
Let’s get started with a review of the current recommendations and challenges. Here we go.
At this time, there are no consensus recommendations for the perioperative management of SGLT2 inhibitors. Plus, many of the published recommendations are outdated or based on limited data. Check out Table 1 in the article for a Summary of Current Notable Recommendations on Perioperative SGLT2i Use.
The 2020 Anesthesiology article recommended continuing SGLT2 inhibitors for ambulator surgery, but holding this medication on the morning of surgery based on expert opinion. Also in 2020, the United States Food and Drug Administration published recommendations to hold SGLT2 inhibitors for at least 3-4 days before all scheduled surgery. These recommendations were based on limited case reports and the elimination half-life of SGLT2 inhibitors. The American Association of Clinical Endocrinologists and American College of Endocrinology recommendations were first published in 2016 and then updated in 2020 and included immediate cessation prior to emergency surgery and holding for 24-48 hours before elective surgery based on case reports and expert opinion. Fast forward to 2023 and the FDA recommendations were evaluated by reviewing 99 reported cases of SGLT2 inhibitor associated diabetic ketoacidosis. None of these cases were in patients who held their medication for longer than 3 days. For these reviewed cases, only about 58% discontinued their SGLT2 inhibitors preoperatively and none of the reviewed cases stopped their medication for more than 2 days preoperatively. Following this, the FDA recommendations were adopted by several organizations.
What is happening here? Why is there a lack of evidence when it comes to the perioperative management of SGLT2 inhibitors? There are several factors. First and most concerning is that the presentation of the associated euglycemic ketoacidosis is atypical so it is likely underreported which leads to challenges with understanding the prevalence and impact on perioperative outcomes. If we look at the literature outside of the perioperative space, there are two large meta-analyses that assessed 82 randomized controlled trials which revealed that SGLT2 inhibitors are not significantly associated with a higher risk of diabetic ketoacidosis compared to other hypoglycemic medications. The American Association of Clinical Endocrinologists and the American College of Endocrinology have stated that the risk of diabetic ketoacidosis associated with SGLT2 inhibitors is no greater than the low levels that occur in patients with diabetes. Keep in mind that these studies and position statements make no mention of the risk of euglycemic ketoacidosis which has a different clinical presentation, diagnostic criteria, and occurrence rate. So, why does perioperative SGLT2 inhibitor administration increase the risk for euglycemic ketoacidosis compared to other hypoglycemic medications? What is so special about these medications and are there other perioperative factors that affect the risk of developing this complication? We might not have all the answers, but it’s time to dive into the literature for a review of the recent updates on perioperative SGLT2 inhibitor use.
Here we go. In 2022, the first and largest population-based study examining the incidence of SGLT2 inhibitor-associated postoperative diabetic ketoacidosis was published and included almost 150,000 patients with type 2 diabetes over a 5 year time period. The incidence of postoperative diabetic ketoacidosis within 30 days was 6 times higher in patients taking SGLT2 inhibitors compared to those not taking this medication. In addition, patients taking SGLT2 inhibitors who developed diabetic ketoacidosis had higher rates of complications include need for mechanical ventilation, infection, and hospital length of stay and an overall increased mortality. The big takeaway is that this is the first study to establish SGLT2 inhibitor use as an independent risk factor for developing postoperative diabetic ketoacidosis. There were some limitations to this study:
No uniform diagnostic criteria for diabetic ketoacidosis
No confirmation of euglycemic presentation.
It is important to keep in mind that SGLT2 inhibitors can cause prolonged glycosuria and ketonemia for up to 9-10 days after stopping the medication so this can be a confounding factor.
Let’s fast forward to 2023 and a single institution retrospective analysis published in the British Journal of Anesthesia. This study included 463 patients on SGLT2 inhibitors and found that all patients on these medications after holding for 1.5 days developed some degree of ketoacidosis with a mean increase in anion gap from 12.6mmol/L preop to 13.4 mmol/L postop. The authors concluded the following: An anion gap acidosis, likely from ketoacids, develops in all patients who do not hold their SGLT2 medication preoperatively. If the medication is not stopped, then postoperative monitoring of the anion gap and serum ketones can help identify patients with euglycemic diabetic ketoacidosis and this is particularly important for patients undergoing emergency surgery. I will include the citation in the show notes so that you can check out the article in detail. The authors of the APSF article highlight that without clear diagnostic criteria to differentiate the types of ketoacidosis, it remains difficult to understand the incidence and impact of this complication and thus develop evidence-based perioperative guidelines for patients taking SGLT2 inhibitors.
With that literature review, it’s time to discuss practical practice considerations and recommendations. Let’s check out Table 2 in the article for risk factors for the development of perioperative SGLT2 inhibitor-associated euglycemic ketoacidosis. These include the following:
- Underlying comorbidities such as female sex, Advanced or poorly controlled T2DM. (Recently, a HgbA1c >8% was reported to cause 3.1-fold increased risk.), Liver disease, Concomitant insulin use which was recently reported to cause 2.8-fold increased risk, and Obesity.
- Surgical type including emergency, bariatric, and cardiac. Emergency surgery has been reported to increase the risk by almost 25%.
- And Other perioperative considerations such as Pre- and Postoperative hypovolemia, Postoperative nutrition since inadequate nutrition can worsen postoperative catabolic state and worsen metabolic complications, Infection/sepsis due to impaired adequate glycemic control and physiological stress, and Glucocorticoid use which can promote hyperglycemia and insulin resistance.
Let’s take a look at the guidelines that were developed by the University of Pennsylvania to incorporate the following factors.
Anticipated procedure duration
Anaesthesia type
Preoperative HgbA1C, glucose, and basic metabolic panel
And underlying patient comorbidities
The guideline continues to use the FDA recommendation for preoperative SGLT2 inhibitor cessation and needs further optimization, but it is the first published approach to develop an algorithm to guide the management of high-risk euglycemic ketoacidosis cases that anaesthesia professionals can use to provide safe anaesthesia care for patients taking SGLT2 inhibitors.
We also need to consider that for some patients, the risks of holding their SGLT2 inhibitor outweighs the benefits. The EMPEROR trial revealed a cardioprotective benefit for taking empagliflozin and the patients that were prospectively withdrawn from treatment had an increased risk of cardiovascular death and hospitalization for heart failure within 30 days of discontinuation back to their pretreatment baseline. Since there is a rapid reversal of the cardioprotective benefits of SGLT2 inhibitors, some advocate for early detection and treatment of ketoacidosis with intraoperative lab monitoring for acidosis and insulin infusion use instead of perioperative discontinuation of SGLT2 inhibitors in patients with heart failure. For patients taking SGLT2 inhibitors for cardiorenal indications who do not have type 2 diabetes, they should continue to take their medication perioperatively since there is no increased for euglycemic ketoacidosis in these patients.
The authors recommend using a perioperative algorithm for patients taking SGLT2 inhibitors and we are going to check out Figure 1 in the article which I will include in the show notes. Keep in mind that this is an area that is lacking evidence in the current literature and this algorithm may not apply in every case.
The first step is to hold SGLT2 inhibitors for 3 days prior to elective surgery, except for patients with significant history of heart failure or patients without type 2 diabetes taking SGLT2 inhibitors for cardiorenal protection. And 4 days for patients taking Ertugliflozin.
Okay, so what do we go if patients do not hold their medication appropriately.
If it is an elective procedure, the next step is to assess for risk factors for DKA. Remember, these risk factors include
- Advanced or poorly controlled type 2 diabetes with HgbA1c greater than 8%
- Liver disease
- Obesity
- Type of surgery including bariatric or cardiac
- Poor nutritional status
- Significant preoperative hypovolemia
- Underlying infection or sepsis
- Glucocorticoid use
For patients without risk factors, the patient is low risk for DKA and can proceed with surgery in the following cases:
- The use of MAC, local, or regional anaesthesia
- Duration of anaesthetic less than 1 hour
- Anticipated return to baseline nutritional intake postop
- No other significant comorbidities
For patients at high risk for the development of DKA, if you can, reschedule the surgery with appropriate outpatient follow-up and proper instruction on SGLT2 inhibitor hold time.
If you can’t reschedule the surgery, head over to the emergent, urgent surgery pathway.
For patients who did not hold their SGLT2 inhibitor appropriately who need to undergo emergent or urgent surgery that cannot be re-scheduled, recommend proceeding with surgery, but consider the following.
- Preoperative basic metabolic panel to check glucose and anion gap
- Continue close intraoperative monitoring for glucose and acidosis
- Intraoperative insulin infusion use
- Close postoperative monitoring for DKA at advanced level of care until return to adequate nutritional intake
Remember, for non-diabetic patients taking SGLT2 inhibitors for heart failure or cardiorenal protection, this algorithm likely does not apply and based on the current available data, they should continue SGLT2 inhibitors and are considered low risk for the development of diabetic ketoacidosis.
These patients may require close perioperative monitoring for acidosis depending on other confounding risk factors.
The authors leave us with the following call to action:
“We believe that SGLT2 Inhibitors pose an increased risk for diabetic ketoacidosis and other morbidities in the perioperative setting. However, the optimal preoperative hold time for these medications and how cases should be handled if the hold time is not met remains controversial. Anaesthesia professionals must remain vigilant since many patients do not adhere to a universal hold time or may not follow preoperative instructions. While further research is needed, we encourage clinicians to consider the currently reported risk factors, along with other patient and surgical factors, to risk-stratify and individualize the management of patients taking SGLT2i, from case cancellation consideration to enhanced postoperative monitoring.”
Do you have a protocol that you follow at your institution for patients taking SGLT2 inhibitors? If not, you may consider using this algorithm which you can find in the show notes. This is an important way that anaesthesia professionals can help to keep patients taking SGLT2 inhibitors safe during and after anaesthesia care.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
Thanks for listening. If you enjoy listening to the Anesthesia Patient Safety Podcast, and we hope that you do, please take a minute to give us a 5-star rating, subscribe, and share this podcast with your colleagues and anyone you know who is interested in anesthesia patient safety.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
