Episode #243 Unlocking Insights for Safer Anesthesia: Key Findings from the Literature and a Case Report
February 26, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Today, we are returning to the In the Literature column to review a couple more articles.
Our first featured APSF summary today was written by Mershon and published on January 27th, 2025. The article was published in Pediatric Anesthesia in August 2024. It is “Spontaneous recovery from neuromuscular block after a single dose of a muscle relaxant in pediatric patients: A systematic review using a network meta-analytic and meta-regression approach” written by Vanlinthout and colleagues.
Our next In The Literature summary was completed by Ehrenwerth and published on February 3, 2025. The article is “Evaluation of a Novel Adjunct to Facilitate Tracheal Intubation,” by Zarnegar and colleagues and published in Anesthesia and Analgesia November 2024.
It’s time to check out the Articles Between Issues column. Our next featured article is “Case Report: Needle Thoracostomy: The Right Equipment for the Job?” by Samuel George and colleagues. This article was published online August 8, 2024.
Check out Figure 1 in the article for a picture of the anti-reflux valves that can be found in many IV catheters.
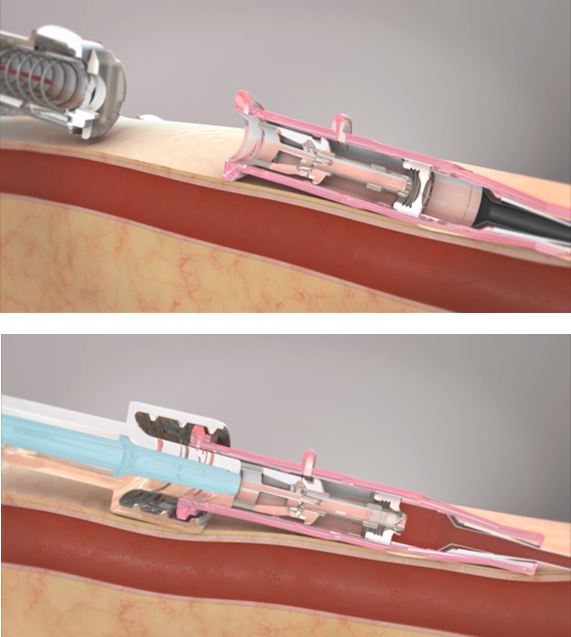
Figure 1: The top picture demonstrates a closed septum with the anti-reflux valve closed inside a BD Insyte Autoguard BC Pro IV catheter when the needle is withdrawn after placement. The bottom picture demonstrates an open septum of the anti-reflux valve when a a Luer-lock mechanism is attached to the IV catheter hub.4
The deadline for the June 2025 APSF Newsletter is right around the corner on March 1st! Check out the guide for authors over at APSF.org for more information.
https://www.apsf.org/apsf-newsletter/guide-for-authors/
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Last week, we explored the APSF’s In the Literature section and reviewed several articles with hot topics including the following:
- Perioperative diabetes management for ambulatory surgery
- How fatigue may impact patient safety
- GLP-1 receptor agonists and residual gastric content
- And the use of methadone for next-day discharge surgery with opioid-sparing benefits.
If you haven’t listened to episode #242 already, what are you waiting for? We hope that you will check it out.
Before we dive further into the episode today, we’d like to recognize Medtronic, a major corporate supporter of APSF. Medtronic has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Medtronic- we wouldn’t be able to do all that we do without you!”
Today, we are going to return to the In the Literature column to review a couple more articles.
First up, we have a very interesting article related to pediatric anesthesia. The APSF summary was written by Mershon and published on January 27th, 2025. The article was published in pediatric anesthesia in August 2024. It is “Spontaneous recovery from neuromuscular block after a single dose of a muscle relaxant in pediatric patients: A systematic review using a network meta-analytic and meta-regression approach” by Vanlinthout and colleagues. To follow along with us, head over to APSF.org and click on the Patient Safety Resources Heading. The seventh one down is In the Literature. Then, scroll down until you get to our featured article. I will include a link in the show notes as well.
This is an important article whether you are a pediatric anesthesiologist or provide anesthesia care for pediatric patients as part of your practice. Here we go.
For a bit of background, the administration of a single dose of neuromuscular blockade is common for pediatric patients undergoing general anesthesia. Even with a single dose, there are important considerations related to age ranges and pharmacokinetic and pharmacodynamic variations that can have a big impact on perioperative outcomes in children. Keep in mind that there is a higher risk for postoperative residual curarization in children due to their unique pharmacokinetic and pharmacodynamic profiles. The investigators completed a systematic review and meta-analysis of 71 randomized controlled trials and controlled clinical trials with over 4300 patients to evaluate the time to neuromuscular recovery following single-dose administration of different neuromuscular blocking agents across pediatric age groups.
Here are the results from the meta-analysis:
There was a faster recover from neuromuscular blockade in children aged 2-11 years old compared to neonates age less than 28 days and infants age between 28 days to 12 months.
There was a log-linear relationship between the dose and duration of neuromuscular blockade. Thus, higher doses led to longer block duration.
The use of volatile anesthetic agents led to a 30-50% increased duration of neuromuscular blockade especially in younger patients who are more sensitive to these agents.
The impact of volatile anesthetic agents on prolonged recovery from neuromuscular blockade is age and time-dependent. Children younger than 3 years old required more time to recover from the blockade when volatile agents were administered compared to older children receiving the same anesthetic agents and neuromuscular blocker.
There was significant interindividual variability which means that it is critical for anesthesia professionals to use quantitative monitoring to prevent residual blockade. This is especially important for pediatric patients since many of the surgical procedures are shorter in duration.
Monitoring neuromuscular blockade may be difficult in children. Acceleromyography may not be very reliable.
The authors conclude with the following recommendations:
- When possible, avoid using neuromuscular blocking agents for pediatric patients.
- Tailor the dose based on the patient’s age.
- Keep in mind that a lower weight-adjusted doses may be needed for younger patients to avoid prolonged recovery.
- Accurate quantitative neuromuscular monitoring should be used to adequately assess recovery. This is important even after one single dose.
- For shorter surgeries or when rapid recovery is needed, the use of shorter-acting neuromuscular blockers like mivacurium or cisatracurium may be helpful.
- Total intravenous anesthesia or TIVA may reduce the impact of volatile agents on recovery from neuromuscular blockade especially for infants and neonates.
That was a great article to review and a very helpful summary. Do you need to make any changes to your practice? These are important considerations to help keep pediatric patients safe when neuromuscular blocking agents are used during anesthesia care.
We are moving on to our next In the Literature summary. What if there was a new tool that could be used to help with one of the most fundamental procedures for anesthesia professionals, tracheal intubation? Well, our next In the Literature summary was completed by Ehrenwerth and published on February 3, 2025. Our article is “”Evaluation of a Novel Adjunct to Facilitate Tracheal Intubation,” by Zarnegar and colleagues and published in Anesthesia and Analgesia November 2024. You can follow along by scrolling up from our last summary and I will include a link in the show notes as well.
Have you used a video-laryngoscope recently? I just used one this week to help facilitate tracheal intubation. Despite the advantages of video-laryngoscopy, it is important to be careful with the metal stylet which may cause bleeding and tissue damage. Just because you have a better view of the glottis does not necessarily mean that you will be able to place the endotracheal tube into the trachea with video-laryngoscopy. But, what if there was new stylet with a flexible tip that could be adjusted by the user using their thumb. This is exciting! Let’s take a look at the study that evaluated this novel device. I will include a picture of this device in the show notes as well.
The study involved 8 anesthesiologists with an average of 15 years experience. The participants watched a 75 second training video and then each anesthesiologist immediately performed 4 laryngoscopies and intubations on a manikin. The four intubations included using a standard Macintosh blade, a video laryngoscope with a metal stylet, a video laryngoscope with a standard bougie, and a video laryngoscope with the new flexible tip stylet. The results revealed that the time to intubation was slightly less with the new flexible intubation aid. All of the participants scored that device as very easy or easy to insert into the larynx and trachea. Compared to the metal stylet, the new stylet was much easier or easier for 7 out of the 8 participants. All 8 participants favoured the new stylet compared to the bougie. Two participants who do not use video laryngoscopy often were unsuccessful with the metal stylet, but were able to intubate with the new stylet. This study provides a glimpse into a new tool that may be used to keep patients safe during intubation with a video laryngoscope and the new flexible intubation aid.
We made it to the top of the In the Literature column, but not the end of the show. It’s time to check out the article between issues column. Our next featured article is “Case Report: Needle Thoracostomy: The Right Equipment for the Job?” by Samuel George and colleagues. This article was published online August 8, 2024. To follow along with us, head over to APSF.org and click on the Newsletter heading. The second one down is Articles Between Issues. From here, scroll down until you get to our featured article today and I will include a link in the show notes as well.
Have you ever had to perform a needle thoracostomy for a tension pneumothorax? This is something anesthesia professionals learn about during training and in simulation, but rarely if ever need to do. A needle decompression can be performed with a large-bore IV catheter between 10-16gauge along the second-third intercostal space along the mid-clavicular line. This article reports on a successful needle thoracostomy that was complicated by using an intravenous catheter that contained an anti-reflux valve. Anti-reflux valve were first added to intravenous catheters in the 1980s to decrease blood exposure during IV placement and to prevent against infection and accidental needle sticks with an integrated needle retraction mechanism. There are a lot of benefits associated with anti-reflux valves but they may lead to delayed recognition of a successful need thoracostomy. Check out Figure 1 in the article for a picture of a BD Insyte Autoguard BC Pro IV catheter with a closed septum with the anti-reflux valve after the needle has been withdrawn. The bottom picture reveals the open septum when a luer-lock mechanism is attached to the hub. I will include this picture in the show notes as well.
Let’s look at the case. A 69 year old woman with a history of chronic obstructive pulmonary disease underwent bronchoscopic lung volume reduction surgery with insertion and removal of Zephyr valves under general anaesthesia with an endotracheal tube. She was extubated and brought to the PACU. In the PACU, the patient was tachycardiac (HR 120s) and hypotensive with a blood pressure of 80/50mmHg, and hypoxemic with SpO2 in the low 50s and a fast respiratory rate with increased work of breathing. The patient was reintubated emergently and found to have absent right breath sounds. A tension pneumothorax was at the top of the differential diagnosis. An immediate needle thoracostomy at the 2nd rib at the midclavicular line was performed with a 4.77cm 18 gauge IV catheter. There was no rush of air, so the first 18g catheter was removed and a 16 g IV catheter was placed at the same spot. Once again there was no audible rush of air. Finally, a 4.49cm 14-gauge IV catheter was placed with subsequent audible release of air, deflation of the right hemithorax, and immediate improvement in oxygen saturation. Upon inspection of the 18g and 16g IV catheters, these were both found to have the integrated anti-reflux valves which was not present in the 14 g catheter. A chest tube was placed by the interventional pulmonologist in the PACU and a chest Xray revealed only a small residual pneumothorax. The patient was extubated later that day and discharged home three days later with complete resolution of her pneumothorax.
The authors provide some helpful insight following this case. There was delayed recognition of successful decompression because of the anti-reflux valves which prevented the release of air. It may have been helpful to attach a syringe to the catheter after withdrawing the needle to attempt aspiration of air. The syringe would have opened the anti-reflux valve and allowed the team to assess the attempted decompression. Ultrasound may have been useful in this case as well. At the author’s institution, this case was discussed with the departmental quality committee and the director of simulation who proposed the following changes:
- Ensure that there are 14-gauge valveless IV catheters in PACU for use in future situations
- Implement needle decompression in educational resident simulation sessions via practicing on mannequins. Participants would use IV catheters containing and not containing anti-reflux valves for needle decompression and observing if there is a difference in the speed of recognition of successful decompression between catheters with and without anti-reflux valves
Thank you to authors for presenting this interesting case. The big takeaway is that anti-reflux valves may delay recognition of a successful pneumothorax decompression.
That’s all the time we have for today and it was a big day for reviewing neuromuscular blockade in pediatric patients, a novel flexible intubation aid for use with video laryngoscopy, and tips for successful needle decompression. Next week, we’ll be back with a new show from the all-new February 2025 APSF Newsletter. You can get a head start with the new articles by heading over to APSF.org and clicking on the Newsletter heading. The first one down is the current issue. There is so much to talk about and to learn about as we continue to work towards improved patient safety.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
