INTRODUCTION
Needle thoracostomy for tension pneumothorax is a procedure widely taught in simulation labs but is infrequently used by anesthesia professionals in practice. Successful needle decompression can be accomplished via a large-bore IV catheter, typically size 10-16 gauge along the second to third intercostal space along the mid-clavicular line.1 We present a case of a successful needle thoracostomy performed which was initially complicated by the inadvertent use of intravenous catheters with anti-reflux valves. Anti-reflux valves are a relatively new innovation for intravenous catheters, coming into the market after the 1980’s. Anti-reflux valves decrease blood exposure during intravenous cannulation as well as potentially protect against infection and prevent accidental needle sticks through integrated needle retraction mechanisms.2 These catheters, however, could potentially lead to delayed recognition of successful needle thoracostomy if used.
CASE DESCRIPTION
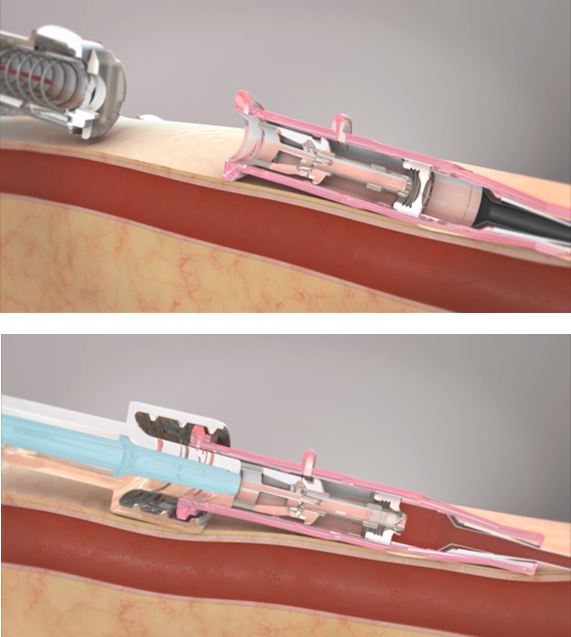
Figure 1: The top picture demonstrates a closed septum with the anti-reflux valve closed inside a BD Insyte Autoguard BC Pro IV catheter when the needle is withdrawn after placement. The bottom picture demonstrates an open septum of the anti-reflux valve when a a Luer-lock mechanism is attached to the IV catheter hub.4
A 69-year-old female with a history of chronic obstructive pulmonary disease underwent bronchoscopic lung volume reduction surgery with insertion and removal of Zephyr® (PulmonX, Redwood City, CA) valves under general endotracheal tube anesthesia. She was successfully extubated in the bronchoscopy suite and brought to the post-anesthesia care unit (PACU). Upon arrival to the PACU, the patient was noted to be tachycardic with a heart rate in the low 120’s, hypotensive with a blood pressure of 80/50, and hypoxemic with SpO2 in the low 50’s and tachypneic with increased work of breathing. The patient was reintubated and immediately after auscultation, absent right breath sounds were noted. A tension pneumothorax was suspected and immediate needle thoracostomy at the second rib of the mid-clavicular line was performed with a 4.77 cm 18-gauge intravenous catheter. No rush of air was heard so the clinician removed the 18-gauge catheter and placed a 16-gauge intravenous catheter. Again, no audible rush of air was appreciated. A 4.49 cm 14-gauge intravenous catheter was obtained and placed in the same location with subsequent audible release of air, deflation of the right hemithorax, and improvement in oxygen saturation.
After successful decompression, it was noted that both the 18- and 16-gauge catheters had integrated anti-reflux valves (BD Insyte Autoguard BC Pro – Franklin Lakes, NJ), whereas the 14- gauge catheter lacked an integrated anti-reflux valve (BD Insyte Autoguard – Franklin Lakes, NJ) (Figure 1).
A chest tube was later placed by the interventional pulmonologist in the PACU, and a subsequent chest x-ray demonstrated a small residual pneumothorax. The patient was then transported to the intensive care unit intubated and sedated. She was extubated later that day and discharged home three days later with complete resolution of her pneumothorax.
DISCUSSION
Needle decompression can be performed using a 10- to 16-gauge IV catheter. It is recommended to attach a Luer-lock syringe on the end of the catheter to confirm placement via aspiration of air.3 In our situation, a tension pneumothorax was diagnosed by physical examination after reintubation for respiratory distress (i.e. unilateral absent breath sounds with persistent hypoxia). Recognition of successful decompression was delayed by anti-reflux valves in IV catheters preventing a release of air, which was subsequently immediately seen after using an IV catheter lacking an anti-reflux valve. In retrospect, it may have been helpful to attach a syringe after withdrawal of the needle to the catheters thought to be unsuccessful (i.e. those containing anti-reflux valves) which would have broken the anti-reflux valve and assess the success of our intervention. In addition, the use of ultrasound after the initial needle decompression could have been used to note successful decompression. This case was also discussed in our departmental quality committee and with our director of simulation, and the following changes are being proposed:
- Ensure that there are 14-gauge valveless IV catheters in PACU for use in future situations
- Implement needle decompression in educational resident simulation sessions via practicing on mannequins. Participants would use IV catheters containing and not containing anti-reflux valves for needle decompression and observing if there is a difference in the speed of recognition of successful decompression between catheters with and without anti-reflux valves
In summary, we present a case of delayed recognition of successful needle decompression of tension pneumothorax due to an intravenous catheter containing an anti-reflux valve. While a useful tool for helping to prevent bloodborne pathogen exposure and accidental needle sticks, anti-reflux valves may cause a delay in recognition of successful pneumothorax decompression.
Samuel George, DO is a CA-2 anesthesiology resident in the Department of Anesthesiology at the Medical College of Wisconsin, Milwaukee, WI.
Aakash Saxena, DO is a CA-3 in the Department of Anesthesiology at the Medical College of Wisconsin, Milwaukee, WI.
Aaron Sandock, MD is a CA-3 anesthesiology resident in the Department of Anesthesiology at the Medical College of Wisconsin, Milwaukee, WI.
Christine Boxhorn, MD is an assistant professor of anesthesiology in the Department of Anesthesiology at the Medical College of Wisconsin, Milwaukee, WI.
The authors have no conflicts of interest.
REFERENCES
- Aho JM, Thiels CA, El Khatib MM, et al. Needle thoracostomy: Clinical effectiveness is improved using a longer angiocatheter. J Trauma Acute Care Surg. 2016;80(2):272-277. doi:10.1097/TA.0000000000000889
- Rivera, A & Strauss, Kenneth & Van Zundert, André & Mortier, Eric. (2005). The history of peripheral intravenous catheters: How little plastic tubes revolutionized medicine. Acta anaesthesiologica Belgica. 56. 271-82.
- Buchanan A. Needle and Tube Thoracostomy. In: Sherman SC, Weber JM, Schindlbeck MA, Rahul G. P. eds. Clinical Emergency Medicine, 1e. McGraw-Hill Education; 2014. Accessed February 25, 2024. https://accessemergencymedicine.mhmedical.com/content.aspx?bookid=991§ionid=55139112
- BD Insyte Autoguard BC shielded IV catheter animation in-service video. www.bd.com. Accessed June 13, 2024. https://www.bd.com/en-ca/videos/bd-insyte-autoguard-bc-shielded-iv-catheter-animation-in-service
