Episode #240 Enhancing International Anesthesia Patient Safety: Insights on ISO Standards
February 5, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
We are returning to the October 2024 Newsletter once again. Our featured article is “Switchover to ISO 80369-6 (neuraxial applications) in Japan: Lessons Learned from Unwittingly Being First” by Sachiko Omi, MD, PhD; Akito Ohmura, MD, PhD; Katsuyuki Miyasaka, MD, PhD.
Thank you so much to Sachiko Omi for contributing to the show today.
Check out Figure 1 in the article which shows the old standard Luer connector and the new standard, ISO 80369-6, connector.
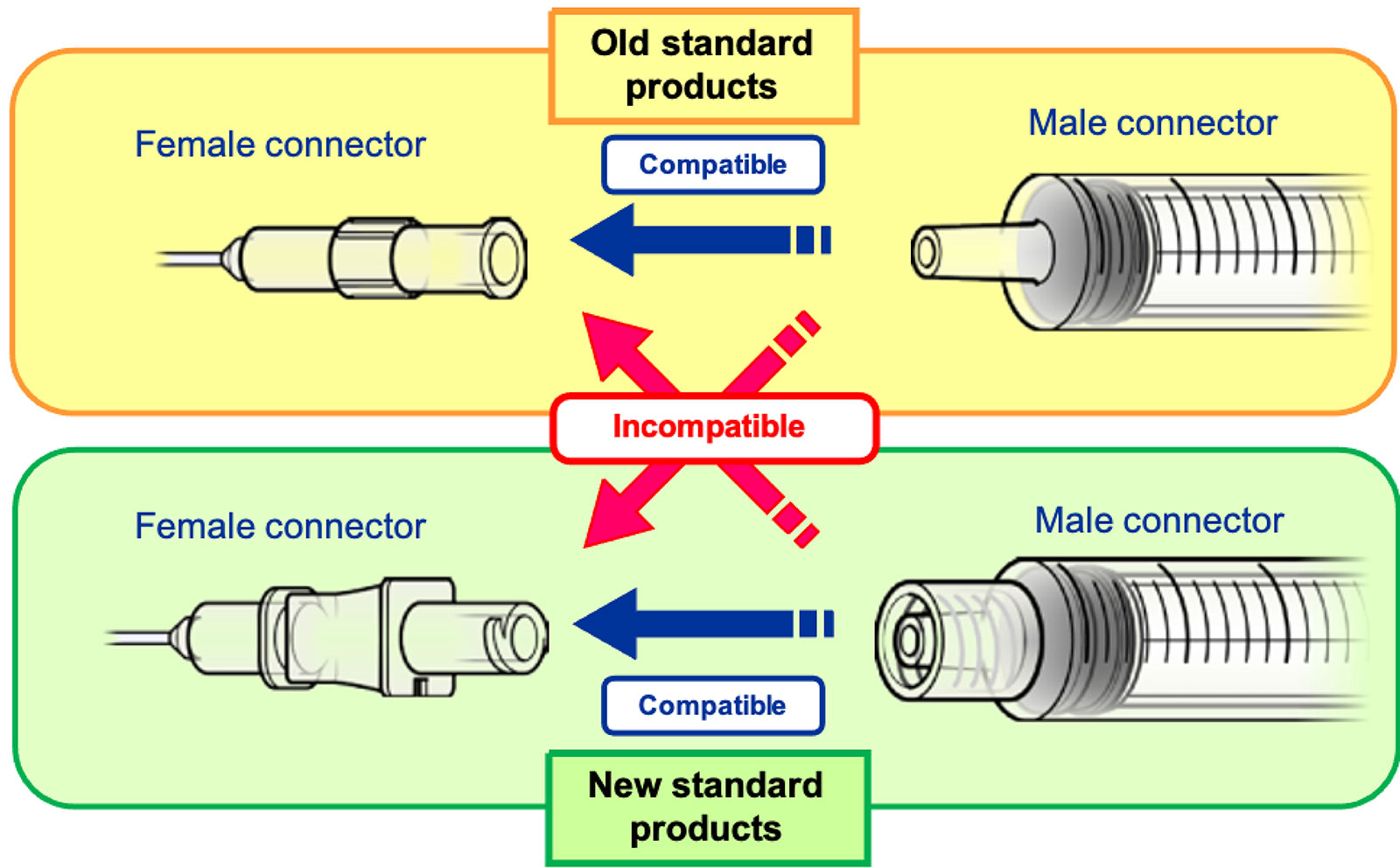
Figure 1: Old standard (Luer) connector and New standard (ISO 80369-6) connector.
PMDA Medical Safety Information, No.55 August 2018, Connections of new and old standard products http://www.pmda.go.jp/english/safety/info-services/safety-information/0001.html
The APSF has made it even easier to stay up to date with the literature on anesthesia patient safety. Head over to APSF.org and click on the Patient Safety Resources Heading. Here you will find the latest in patient safety with summaries of the best medical journal articles from the APSF Newsletter Editorial Board.
https://www.apsf.org/in-the-literature/
This episode was produced by Mike Chan. He joins the APSF team as our podcast editor and producer.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Do you know what ISO stands for? It is the International Organization for Standardization. This organization was established in 1947 as a non-governmental organization in the United Nations to help boost the global economy after World War II with a focus on standardizing industrial products and manufacturing process to help foster international trade. I know what you are thinking…Am I still listening to an anesthesia patient safety podcast? Don’t worry, we will be talking about important anesthesia patient safety considerations, so stay tuned.
Before we dive further into the episode today, we’d like to recognize Vertex, a major corporate supporter of APSF. Vertex has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Vertex- we wouldn’t be able to do all that we do without you!”
We are returning to the October 2024 Newsletter once again. Our featured article is “Switchover to ISO 80369-6 (neuraxial applications) in Japan: Lessons Learned from Unwittingly Being First” by
Sachiko Omi and colleagues. To follow along with us, head over to APSF.org and click on the Newsletter heading. The fourth one down is Newsletter archives. From here, scroll down to the October 2024 Newsletter and then scroll down until you get to our featured article today. I will include a link in the show notes as well.
To help kick off the show today, we are going to hear from the author. Let’s take a listen now.
[Omi] “Hello. I am Sachiko Omi, an anesthesiologist from Japan with 40 years of experience at Tokyo Jikei Medical University. I have recently become aware of ISO and its great impact, for better AND for worse, on anesthesia practice.”
[Bechtel] I asked Omi why did you write this article.
[Omi] “I am well aware of the importance of preventing misconnections to ensure patient safety, but I was unaware of what ISO was doing to address this issue. It happened suddenly, when one day in 2020, out of the blue, I heard the news of how the health ministry of Japan changed the bore sizes of needles and syringes for nerve blocks, spinal anesthesia and epidural anesthesia in accordance with the newly implemented ISO 80369-6 standard. I understood why they made the change, but the introduction of the new standards came without our awareness and without adequate input from clinicians, even within ISO. As a matter of fact, I have experienced several situations where the changes do not necessarily guarantee greater safety. Please read the article for details. We hope listeners from countries around the world will take note of our experience and think about how ISO standards affect them and how they can affect ISO decision-making.
In summary, I wrote this article to raise awareness among clinicians around the world about the workings of ISO.”
[Bechtel] Thank you so much to Omi for helping to contribute to the show today and we will be hearing from him again later. Now, it’s time to get into the article.
The ISO standards for medical devices require input from healthcare professionals working with manufacturers. Manufacturers are often responsible for developing the standards since they have the knowledge and expertise in the manufacturing processes and regulatory compliance. This must be a team effort between clinicians using the devices and manufacturers to meet clinical needs and safety standards. There is a focus on how medical devices are used compared to just their technical specifications. Anesthesia professionals are responsible for using medical devices correctly to keep their patients safe. When there is limited involvement by clinicians for the development of these standards, there is a risk for threats to anesthesia patient safety.
Let’s take a look at the example of ISO 80369. This standard was created in response to medical errors from misconnections and misadministration between enteral, respiratory, urinary, blood pressure, neuraxial, and intravenous patient care systems. These medical errors have occurred all around the world and participating countries have been encouraged to adopt these international standards without delay. Table 1 in the article lists the ISO 80369 Standards related to small-bore connectors for liquids and gases in health care applications. The author highlights that the standard related to breathing systems and driving gases was issued in April 2024 but not implemented in Japan. The standard related to enteral and gastric connectors caused multiple problems after implementation in Japan in 2019 since the connectors were smaller in diameter. The standard related to intravenous connectors was revised to be consistent with previously used and readily available intravenous devices so there was no need to make any changes. Today, we are going to highlight ISO 80369-6 related to Neuraxial connectors.
Check out Figure 1 in the article which displays the old and new standard products which are not compatible with each other. I will include this figure in the show notes as well. This standard has been implemented in Japan under governmental leadership with the expectation that this standard would be similarly implemented around the world. There have been no major accidents or mortality reported during the transition period, but there have been many safety concerns. No other country has completed the transition to the new standard at this time so sharing the knowledge of the experience in Japan can contribute to patient safety around the world by highlighting important considerations related to the new standard.
Before moving forward, let’s look back at the need for a new standard for neuraxial applications. The old standard was the luer connection or ISO-594, that was the standard for injections and connecting small-diameter tubing. Luer connections were convenient and used as the universal connector. There is a big threat to patient safety as a result of this convenience. Preventing misconnections and wrong route drug errors relied on vigilance and responsibility by the clinician. We have talked about it before on this show, but we know that human error is an unavoidable cause of medical errors, and it has led to misconnection between different devices and routes of administration. The development for a new standard started in 2005 with the goal of creating new purpose-specific connections with physical non-interfacing mechanisms specific to each application to make misconnection impossible and ultimately to improve safety. ISO 80369 involves the purpose-specific compatibility standards for preventing misconnections. Technical Committee 210, which is focused on quality management, worked with Technical Committee 121 which includes many anesthesia professionals. Unfortunately, the joint working group with input from anesthesia professionals was not effective during this process. There is a history of anesthesia professionals working on technical committee 121 and especially subcommittee 3 to make contributions related to devices used directly by anesthesia professionals including ventilators, oxygen concentrators, and related patient monitors.
Has ISO 80369-6 been implemented where you practice? In Japan, the implementation of this new standard was not discussed with healthcare professionals. The decision-making process involves the Ministry of Economy, Trade, and Industry which oversees general industries and works with ISO followed by the Ministry of Health, Labour, and Welfare which is responsible for medical devices. The process lacks input from clinicians and healthcare professionals.
Once healthcare representatives were made aware of the implementation of the new standard, several safety concerns were raised related to confusion around the change in connectors. There were no meetings with clinicians or the Japanese Society of Anesthesiologists. There was an understanding that Japan, as a member of the World Trade Organization, needed to adopt the ISO standard as the national standard without delay and without making changes that could create international trade barriers. One of the lessons learned is that it is important to consider the risks and benefits in clinical settings before implementing new standards.
On December 29, 2017, there was a notice that the sale of old products affected by ISO 80369-6 needed to stop by the end of February 2020 at the convenience of the manufacturer. For anesthesia professionals in clinical practice at this time, there was very little awareness about the upcoming switchover. This process took two years. In June 2024, the Ministry of Health, Labour, and Welfare reported on the transition which included a postal survey to evaluate product-related issues, rather than patient-safety related issues. Survey participants included anesthesia professionals and the industrial organization, MTJAPAN. 1447 facilities were contacted, and 329 responses were collected.
Let’s take a look at the survey results now. You can find them in Table 2 in the article.
First, let’s look at the time before the switch over and the following issues:
- Awareness which involves failure to convey the rationale for the new guidelines to the clinicians who would be most affected by the change. Anesthesia professionals and academic societies in Japan did not feel strongly that such a change was needed, but they needed to follow the governmental regulations.
- Guidance which highlights that the Medical Technology Association of Japan did not have the product or the clinical information to adequately guide healthcare providers through the transition.
- Product Range was an issue since some manufacturers stopped making certain products during the transition which reduced the range of available products.
- And Translation which involved the mistranslation of neuraxial application as neural anesthesia in Japanese leading to confusion that the change only applied to spinal and epidural anesthesia and peripheral nerve blocks. This left out spinal taps and other therapeutic applications.
Now, let’s review the issues that arose after the switchover.
- Initial and ongoing troubles with breakage that included cracking, leaking, too tight fit, and non-disengagement.
- Errors in drug administration since the connections at the patient side were secured but the medication side was left unchanged. Standard compatible prefilled syringes and plastic ampules were not always available. Having standard compatible and non-compatible aspiration needles to draw up medications available at the bedside increased the risk of errors.
- Different feel in use during clinical practice related to fitting force, injection pressure, and loss of resistance meaning that anesthesia professionals needed to adapt their practice quickly during the switchover. Advice from the manufacturer was to use the product carefully to avoid cracking which was not particularly helpful in clinical practice.
- Hard to differentiate between lock and luer connectors due to the smaller size of the syringe tip and the use of covers to protect the mechanical weaknesses.
- Color confusion since yellow was associated with the new standard but had previously been used for enteral connections in Japan.
- Less convenient and more complicated procedures
- Increased cost related to disposal of old product stock, inadequate reimbursement of the newer much more expensive products, additional storage space for the increased number of new products, and increased cost of producing multiple narrowed specific product lines
- And finally, lack of systems for product reporting and support with no established system for reporting issues, sharing information, or providing guidance on handling mechanical or clinical problems.
Whew, that is quite a list of issues, and we still have more to discuss when it comes to making the switchover to the new standard including clinician involvement, imbalanced perspectives, lack of clinical feasibility trials, and lack of transparency. We will be back next week to continue the conversation. Plus, we are going to hear from the author again.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
The APSF has made it even easier to stay up to date with the literature on anesthesia patient safety. Head over to APSF.org and click on the Patient Safety Resources Heading. The fourth one down is the In the Literature section. Here you will find the latest in patient safety with summaries of the best medical journal articles from the APSF Newsletter Editorial Board. In addition to listening to this podcast, you can review these in the literature summaries and become a leading voice for anesthesia patient safety at your institution. Some of the topics include perioperative blood glucose management for adult patients undergoing surgery, Effect of fatigue on anesthetist well-being, and GLP-1 receptor agonist use and residual gastric content before anesthesia care. We hope that you will check it out.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
