Episode #237 Preventing Pediatric Medication Errors
January 15, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article is from the October 2024 APSF Newsletter. It is “Pediatric Perioperative Medication Errors” by Ying Eva Lu-Boettcher, MD and Rahul Koka, MD.
Citation:
- Nanji KC, Patel A, Shaikh S, et al. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. 2016;124:25–34. PMID: 26501385
Check out Figure 3 in the article. It displays the bow-tie analysis of intraoperative medication errors. It is important to consider specific evidence-based mitigation techniques to help decrease and prevent medication errors during pediatric anesthesia care.
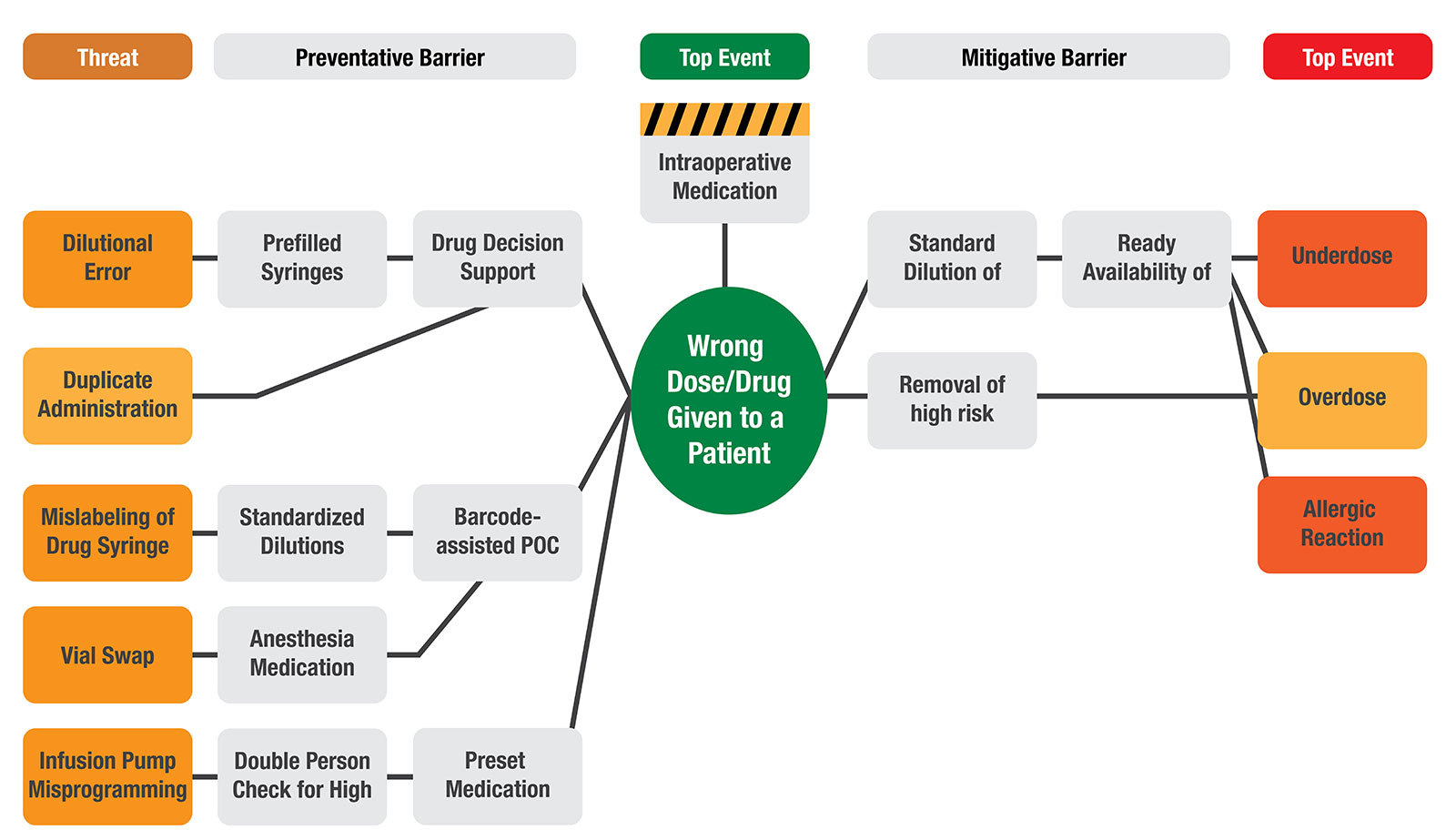
Figure 3: Bow-tie Analysis of Intraoperative Medication Errors.
POC = Point-Of-Care
We hope that you will check out the APSF Technology Education Initiative Courses. Remember these are free of charge and you can earn CME. You can get started over here: https://www.apsf.org/apsf-technology-education-initiative/
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Let’s start with the definition of a medication error. This is a failure in the treatment process that leads to or has the potential to lead to harm to the patient. Have you been involved in a medication error event? It is likely that perioperative medication errors are not always reported. It may be difficult to determine the actual incidence of these events which would rely on reporting by the anesthesia professional as well as direct observation of anesthesia professionals during medication ordering, preparation, and administration. The 2016 Anesthesiology study by Nanji and colleagues was a prospective observational study that revealed a 5.3% incidence of medication errors by direct observation compared to the self-reported incidence of 0.004%. During pediatric anesthesia care, the incidence of self-reported medication errors is between 0.01 and 1.92%. Pediatric patients are at higher risk for medication errors and at higher risk for harm from these errors due to the large variations in body weight and high variability in dosing calculations. This is an area where anesthesia professionals must remain vigilant to protect patients from medications errors during anesthesia care.
Before we dive further into the episode today, we’d like to recognize Fresenius Kabi, a major corporate supporter of APSF. Fresenius Kabi has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Fresenius Kabi – we wouldn’t be able to do all that we do without you!”
We are returning to the October 2024 Newsletter today. You may have already guessed that our featured article is “Pediatric Perioperative Medication Errors” by Eva Lu-Boettcher and Rahul Koka. To follow along with us, head over to APSF.org and click on the Newsletter heading. The first one down is the current issue. From here, scroll down until you get to our featured article today. I will include a link in the show notes as well.
We are going be hearing from both of the authors as we discuss this article. Here is one of the authors now.
[Lu-Boettcher] “ Hi, my name is Eva Lou Boettcherr, a pediatric anesthesiologist at the University of Wisconsin in the United States. I am the Director of Anesthesia Quality and Safety at the Children’s Hospital.”
[Bechtel] I asked Lu-Boettcher why she wrote this article. Let’s take a listen to what she had to say.
[Lu-Boettcher] “ Medication error is an incredibly important topic in our profession.
Anesthesia professionals work under high intensity conditions where multiple doses and classes of drugs are given during fast paced clinical scenarios. More often than not, we are working alone to accomplish these tasks. This is a unique workflow that does not exist in other parts of the medical system.
I wanted to provide evidence based updates on where there are points of vulnerability that could potentially result in patient harm and highlight the pediatric population who are particularly susceptible to our medication errors due to large variations in body weight resulting in high variability in dosing calculations.
Importantly, there have been recent advances in medication error mitigation strategies. I wanted to bring those forward to our readers so that we, as a community, could stay up to date on this topic.”
[Bechtel] And now it’s time to hear from the next author. I will let him introduce himself and tell us why he contributed to this article.
[Koka] “Hello, my name is Rahul Koka. I am a Pediatric Anesthesiologist at the Johns Hopkins Children’s Center in Baltimore, Maryland, where I also serve as the Surgical Director for Quality. Well, being involved in the Wake Up Safe collaborative, I hear of the good work that is being done at other institutions, and I wanted to make sure this knowledge is disseminated. This article was one method of doing that. But, we wanted to provide not just an overview of the most common causes for pediatric medication errors, but to provide some sort of representation that can help providers understand the relationships between causes and risks. We chose to show this relationship through what’s called a bowtie analysis, so that providers can see what preventative treatment is and what mitigative barriers are currently being used at other hospitals and what may be missing from their own practices. I’ll bet that almost every anesthesia provider either knows someone who has made a medication error or has made a medication error themselves. Now, not all these errors have necessarily led to patient harm, but drawing up and delivering a medication is one of the most repeated tasks that we perform during surgery every single day.”
[Bechtel] Thank you so much to Lu-Boettcher and Koka for helping to kick off the show today. And now, it’s time to get into the article.
Medication errors are a big threat to anesthesia patient safety. It is no wonder since the work environment is intense with multiple doses and classes of drugs that need to be administered at the correct time. Plus, anesthesia professionals are responsible for the entire drug administration process from prescribing to preparation to administration to monitoring for effects. With this great responsibility comes some significant hazards. Check out Figure 1 in the article and we are going to review the different medication errors that may occur in the three phases of handling.
Prescribing errors or provider knowledge gap include wrong drug, wrong dose, and allergy.
Preparation Error in non-prefilled syringes include labelling error and vial swap.
Administration Errors may include the following: wrong dose, syringe sway, duplicate administration, omission, overdose, wrong infusion rate, wrong time/route/patient, and expired medication
Just by hearing these lists, you can probably guess which phase has the highest incidence of medication errors. Here are some quick data facts brought to you by Wake Up Safe, a national pediatric anesthesiology quality collaborative:
- The most common medications that result in medication errors are sedatives, hypnotics, and opioids.
- The highest incidence of medication errors occur during the administration phase at 65% with prescribing next at 24 % and finally preparation at 11%.
- If we break down the administration phase, the most common type of error is wrong dose followed by syringe swap which is the accidental administration of the wrong syringe.
- 21% of medication errors involved medication infusions.
- And finally, the vast majority, 97% of these medication errors were deemed to be preventable.
The authors ask an important question: “How do we control the risk during medication administration?”
This is a great question that we need to tackle if we hope to decrease medication errors and ultimately prevent them. If we look at this phase very closely, the most critical step during medication administration is once the syringe has been pushed or the infusion started. Once the drug reaches the patient, there may be immediate and irreversible effects. This is the time when we can use technology and process-based interventions to help.
Let’s check out Table 1 in the article.
Here are several technology based interventions:
- Barcode-assisted point of care documentation systems which may include barcode scanning and labelling with audible and visual feedback or cues
- Drug decision support including EMR defaults for drug order sets, EMR defaults for dosages of routinely administered medications, reminders for when the next dose is due, and alerts for drug interactions with associated patient allergies or medical conditions such as renal failure.
Here are several process based interventions.
- Formal and consistent way of organizing medications in the anesthesia workspace. Check out the Anesthesia Medication Template drug organization system. More on this later.
- Standardization of medication trays and drawers.
- Prefilled syringes to help decrease dilution errors.
- Preset medication infusion library.
- Performing documentation prior to administration which may include barcode scanners for identification and documentation of medication in the EMR prior to administration
- Connecting infusions to the most proximal IV port to avoid inadvertent boluses.
- Removal of high risk medications from the electronic medication dispensing cart.
- Verification of drugs with another staff member prior to administration
- Increase accessibility to easy and non-punitive drug error reporting
- High risk medication labelling.
Which of these interventions are you using in your practice?
What about medication errors during pediatric anesthesia care? Are there specific interventions that may be helpful to decrease and prevent medications errors for this higher risk patient population? Let’s check out Figure 3 for some specific, evidenced-based interventions. I will include this figure in the show notes as well. This analysis includes the threats that may lead to medication errors along with preventive barriers or mitigative barriers to help prevent the wrong dose or drug given to a patient as well as an underdose, overdose, or allergic reaction.
For dilutional errors, interventions may include the use of prefilled syringes and drug decision support.
For duplicated administration, drug decision support can be beneficial.
Mislabelling of drug syringe may be prevented by standardized dilutions and barcode assisted point of care.
Vial swaps can be prevented by barcode assisted point of care and using the anesthesia medication template.
Infusion pump mis programming interventions may include double person check for high risk medications and preset medication templates.
Mitigative barriers to help prevent medication errors include using standard dilutions that are readily available as well as removal of high-risk medications.
We have more to talk about when it comes to paediatric perioperative medication errors, and we are going to hear from the authors again so we hope that you will tune in again next week. Spoiler alert, we will be talking about Anesthesia Medication Template (AMT) drug organization system, prefilled syringes, and point of care barcode scanner.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
We are going to be talking about the newest APSF Technology Education Initiatives on an upcoming episode, but before we do you have time to complete the Quantitative Neuromuscular Monitoring course. The course consists of 6 topics designed to empower the anesthesia professional with the knowledge required to safely and effectively use quantitative neuromuscular monitoring. This is aligned with the ASA 2023 Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade. I will include a link to the course in the show notes. We hope that you will also check out the low-flow anesthesia course and stay tuned for the new course on manual external defibrillation, cardioversion, and pacing that will be release soon.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
