Episode #225 Collaborative Guidelines for Safe Anesthesia in OSA
October 23, 2024
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
We are catching up on another great article from the June 2024 APSF Newsletter. Our featured article today is “Society of Anesthesia and Sleep Medicine: Safety of Patients with Obstructive Sleep Apnea in the Perioperative Period” by Mandeep Singh, Jennifer E. Dominguez, Melanie Lyons, Satya Krishna Ramachandran, Bhargavi Gali.
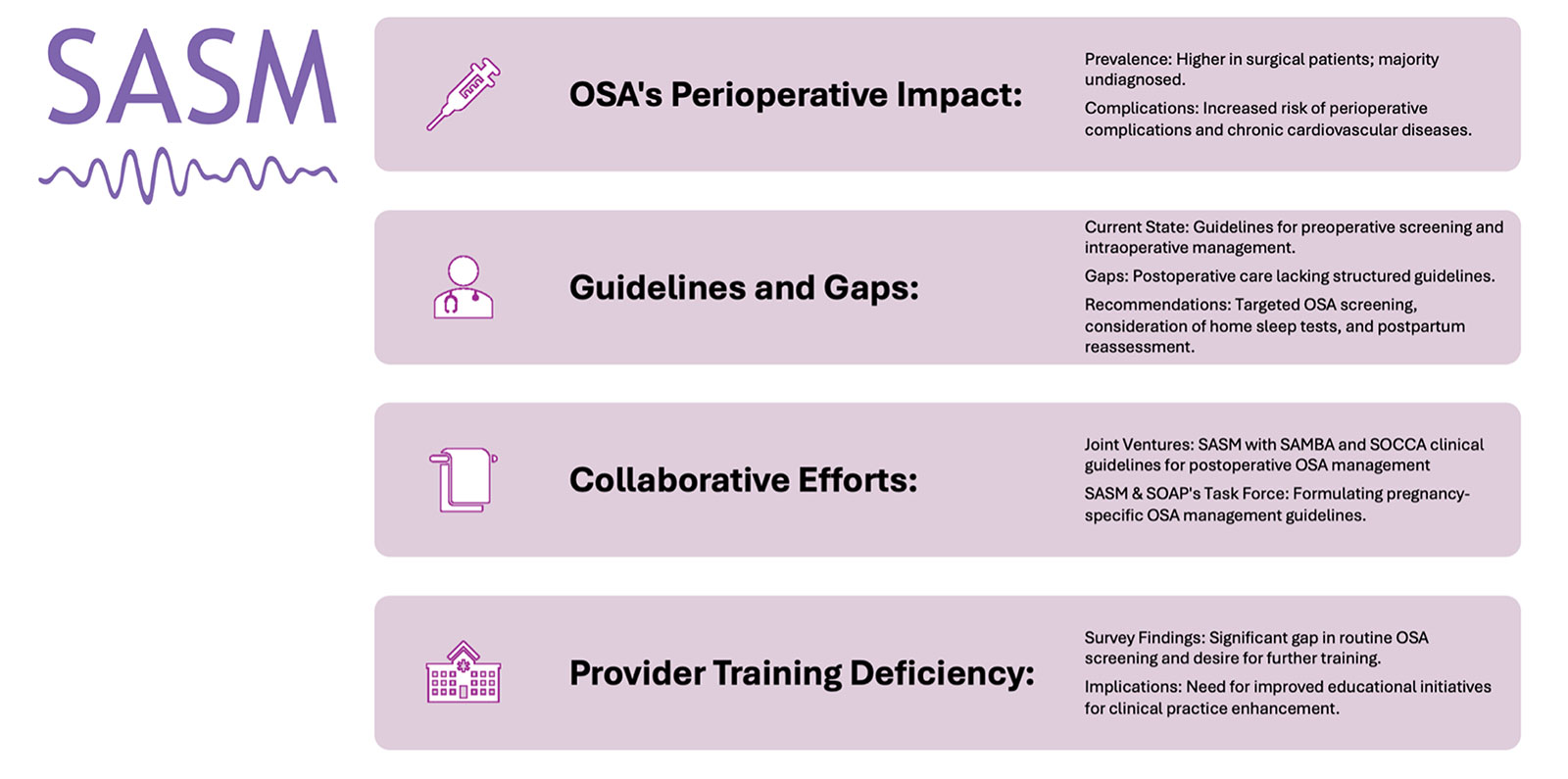
Figure 1: Heeding the “Don’t Look Up'” Call—Society of Anesthesia and Sleep Medicine Leadership, and Collaborative approach to Perioperative Sleep Health Research, and Innovation.
SAMBA: Society for Ambulatory Anesthesia; SASM: Society of Anesthesia and Sleep Medicine; SOAP: Society for Obstetric Anesthesia and Perinatology; SOCCA: Society of Critical Care Anesthesiologists.
Here is the citation to the study about surgical patients with undiagnosed sleep apnea.
- Singh M, Liao P, Kobah S, et al. Proportion of surgical patients with undiagnosed obstructive sleep apnoea. Br J Anaesth. 2013;110:629–636. PMID: 23257990.
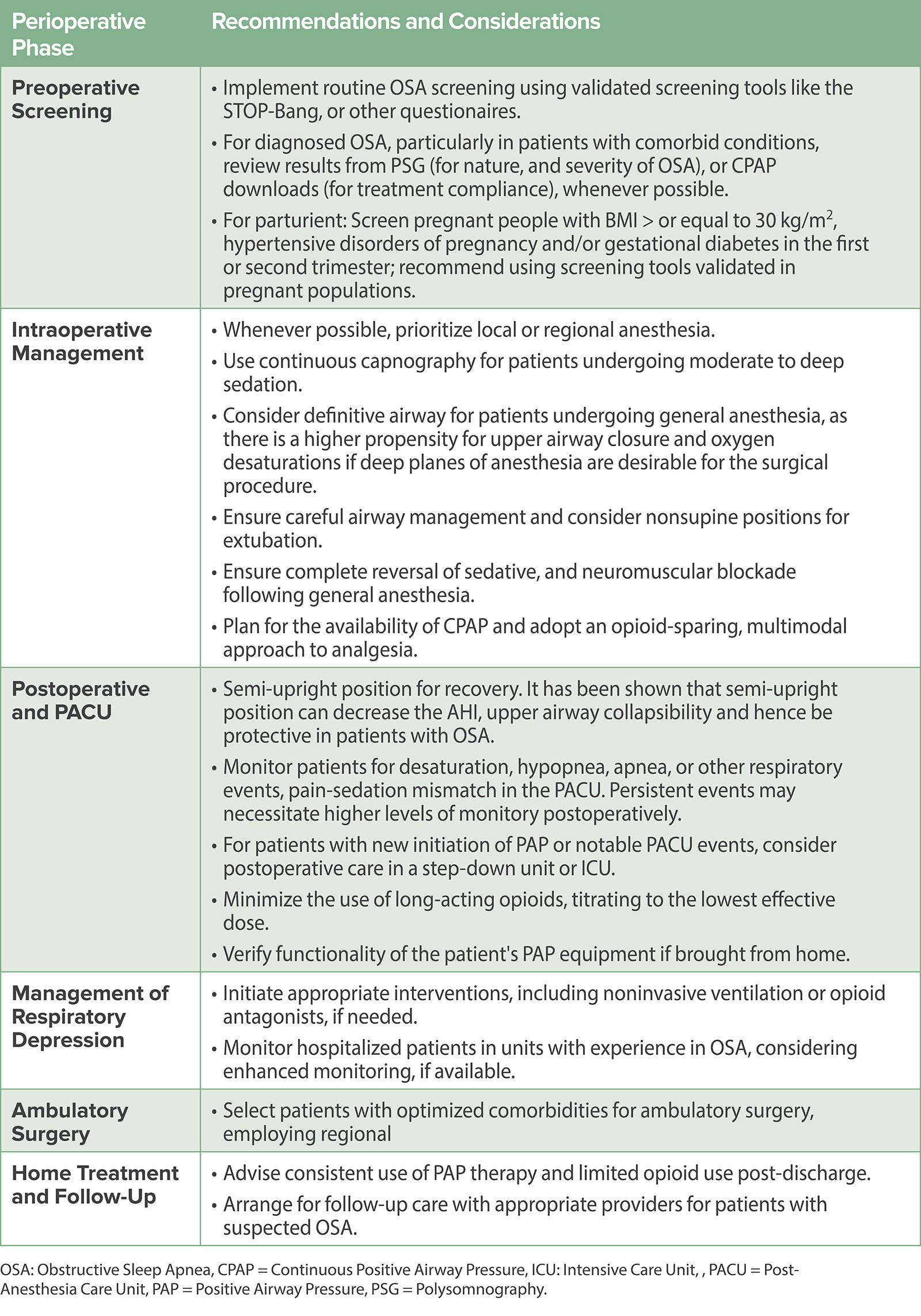
Here is Table 1 from the article with complete recommendations and considerations for providing safe anesthesia care for patients with obstructive sleep apnea from before they even enter the operating room until they are safely home again. This may be a good resource to save on your phone or print out to keep in your anesthesia office.
Check out the SASM and SOAP joint recommendations on the screening, diagnosis, and treatment of patients with OSA during pregnancy including expert opinion where evidence was lacking. These recommendations were published in Obstetrics and Gynaecology in August 2023 (https://journals.lww.com/greenjournal/abstract/2023/08000/society_of_anesthesia_and_sleep_medicine_and_the.22.aspx).28
Have you thought about joining the Society of Anesthesia and Sleep Medicine? For more information check out their website at https://www.sasmhq.org/
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2024, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Do you provide anesthesia care for patients with obstructive sleep apnea? If you are providing anesthesia care for patients undergoing surgery, then you are likely taking care of patients with obstructive sleep apnea or OSA and that means that this show is for you. We are going to be talking about the Society of Anesthesia and Sleep Medicine and reviewing important guidelines related to perioperative care for patients with OSA. So, stay tuned.
Before we dive into the episode today, we’d like to recognize Edwards Lifesciences, a major corporate supporter of APSF. Edwards Lifesciences has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Edwards Lifesciences – we wouldn’t be able to do all that we do without you!”
We are catching up on another great article from the June 2024 APSF Newsletter. Our featured article today “Society of Anesthesia and Sleep Medicine: Safety of Patients with Obstructive Sleep Apnea in the Perioperative Period” by Mandeep Singh and colleagues. To follow along with us, head over to APSF.org and click on the Newsletter heading. Fourth one down is Newsletter archives. Then, scroll down and click on the June 2024 APSF Newsletter. Then, scroll down until you get to our featured article today. I will include a link in the show notes as well.
Have you heard of the Society of Anesthesia and Sleep Medicine? Are you a member? This society, founded in 2010, brings together anesthesia professionals and sleep specialists to focus on keeping patients with sleep disorders safe during the perioperative period. OSA is a risk factor for perioperative complications and the society of anesthesia and sleep medicine is working to address this with research projects and education in the management of patients with OSA and at high risk for undiagnosed OSA. The good news for us is that this work includes the development of guidelines to help provide safe anesthesia care for these high risk patients.
Check out Figure 1 in the article for a depiction of the work being done by the Society of Anesthesia and Sleep Medicine related to Perioperative Sleep Health Research and Innovation and we are going to go through it now.
- The first row describes OSA’s Perioperative Impact. Did you know that the prevalence is higher in surgical patients and the majority of patients are undiagnosed. In addition, these patients have an increased risk for perioperative complications as well as chronic cardiovascular conditions.
- The second row describes the Guidelines and Gaps. The current state includes guidelines for preoperative screening and intraoperative management. The gaps involve postoperative care that lacks structured guidelines. The recommendations from the society are targeted OSA screening, consideration for at home sleep tests, and postpartum reassessment.
- The third row describes the collaborative efforts with the Society for Ambulatory Anesthesia and the Society of Critical Care Anesthesiologists for postoperative management guidelines and with the Society of Obstetric Anesthesia for pregnancy-specific recommendations.
- The final row describes provider training deficiency which includes the following:
- From survey data, significant gap in routine OSA screening and desire for further training
- There is a call to action for improved educational initiatives for clinical practice enhancement.
Wow, we can see that this society is hard at work to improve anesthesia patient safety for patients with OSA and there is work to be done. The good news is that we have some clinical guidelines to help guide you in the management of patients with OSA to keep them safe during the postoperative period.
Here we go.
Remember, obstructive sleep apnea is a sleep-related breathing disorder that involves repeated upper airway collapse which may lead to decreased oxygen saturation during sleep and increased risk for chronic cardiovascular diseases. Did you know that there is a higher frequency of OSA in surgical patients compared to the general population? Plus, many patients with OSA will present for surgery without a formal diagnosis of OSA. Let’s check out the results from the 2013 retrospective nested cohort study of 819 surgical patients who underwent laboratory or portable polysomnography. Anesthesia and surgery professionals completed chart reviews to determine a clinical diagnosis of OSA while remaining blinded to the results of the polysomnography. There were 267 patients found to have moderate to severe OSA prior to surgery with testing. 92% had not been diagnosed by surgeons and 60% were undiagnosed by the anesthesia professionals. I will include a link to the study in the show notes as well. The stakes are high to identify patients with OSA prior to surgery since these patients are at higher risk for perioperative complications as well as increased hospital and resource utilization. Evidenced-based guidelines for postoperative management for patients with OSA is important to keep patients safe, ensure appropriate management, and provide adequate post-discharge instructions. Patients with OSA who undergo ambulatory surgery may be at risk for complications after discharge home. For patients who will be admitted to the ward or general care floors, the initial postoperative period involves close observation in the PACU or ICU, but they may be at risk for complications after transfer.
These new guidelines for postoperative management for patients with OSA are brought to us by the Society of Anesthesia and Sleep Medicine, SAMBA, and SOCCA. We already have guidelines for preoperative and intraoperative management of OSA from the Society of Anesthesia and Sleep Medicine as well as SAMBA’s consensus for the ambulatory management of these patients. This next step is to provide a continuum of strategies from preoperative screening to postoperative follow-up.
To do that, let’s take a look at Table 1 in the article for complete recommendations and considerations for providing safe anesthesia care for patients with obstructive sleep apnea from before they even enter the operating room until they are safely home again. I will include this table in the show notes. This may be a good resource to save on your phone or print out to keep in your anesthesia office.
First up, we are going to talk about preoperative screening. Here are the recommendations and considerations.
- Implement routine OSA screening using validated screening tools like the STOP-Bang or other questionnaires.
- For diagnosed OSA patients, particularly those with comorbid conditions, review results from PSG to determine nature and severity of OSA or CPAP downloads for treatment compliance whenever possible.
- For parturient, screen pregnant patients with BMI greater than or equal to 30, hypertensive disorders of pregnancy, and/or gestational diabetes in the first or second trimester using screening tools validated in pregnant populations.
Let’s move into the operating room for intraoperative recommendations and considerations.
- Whenever possible prioritize regional or local anesthesia.
- Use continuous capnography for patients undergoing moderate to deep sedation.
- Consider a definitive airway for patients undergoing general anesthesia since there is a higher risk of upper airway closure and oxygen desaturation if deep planes of anesthesia are desirable for the surgical procedure.
- Ensure careful airway management and consider non-supine positions for extubation.
- Ensure complete reversal of sedative and neuromuscular blockade following general anesthesia.
- Plan for availability of CPAP and adopt opioid-sparing, multimodal approach to analgesia.
The surgery has been completed and it is time to move into the Postoperative Period. Here are the recommendations and considerations.
- Semi-upright position for recovery. This positioning has been shown to decrease the apnea-hyponea index and upper airway collapsibility and is thus protective for patients with OSA.
- Monitor patients for desaturation, hyponea, apnea, or other respiratory events as well as pain-sedation mismatch in the PACU. Persistent events may necessitate higher levels of monitoring postoperatively.
- For patients with new initiation of CPAP or other notable PACU events, consider postoperative care in a step-down unit or ICU.
- Minimize the use of long-acting opioids, titrating to the lowest effective dose.
- Verify functionality of the patient’s CPAP equipment if brought from home.
These recommendations also address the management of respiratory depression throughout the perioperative period. Here we go:
- Initiate appropriate interventions including non-invasive ventilation or opioid antagonists if needed
- Monitor hospitalized patients in units with experience in OSA considering enhanced monitoring if available.
When it comes to ambulatory surgery for patients with OSA, it is critical to select patients with optimized comorbidities for ambulatory surgery and employ regional anaesthesia.
When patients are getting ready for discharge home, it is important to advise consistent use of CPAP therapy and limit opioid use post-discharge. Another important step is to arrange follow-up care with appropriate clinicians for patients with suspected OSA.
Well, that was a lot of excellent information to help guide anaesthesia professionals who provide care for patients with OSA. Are you following these recommendations in your practice? Are there any steps that you can take to improve patient safety?
Another important mission of the Society for Anesthesia and Sleep Medicine is to assess awareness and clinical practices related to patients with obstructive sleep apnea. A multisite survey was conducted with the support of the American Academy of Sleep Medicine Foundation. Here are the details of the survey:
- The sites included 9 prominent academic institutions
- The participants included physicians in training and advanced practice providers in the fields of anaesthesiology, internal medicine, family medicine, surgery, and obstetrics and gynaecology.
- The results included the following:
- Many physicians in training and advanced practice providers reported that training regarding OSA was inadequate.
- Only 51% felt that training was adequate with a breakdown of 82% in anaesthesiology, 34% in surgery, and 12% in obstetrics and gynaecology with 77% across all specialities desiring additional training.
- Participants were asked about training to assess OSA in the perioperative period and only 38% reported adequate training for this with a breakdown of 84% in anesthesia, 33% in surgery, and 15% in O&G. This survey helps to reveal an opportunity for improved clinical practice and training.
We are moving from the operating theatre to the obstetric ward to talk about clinical guidelines for the management of obstetric patients with OSA. This is a threat to patient safety since maternal morbidity is associated with OSA especially with hypertensive disorders of pregnancy and gestational diabetes mellitus. There may be a correlation between maternal OSA and neonatal outcomes including pre-term birth, Apgar scores, and low birth rate, but more studies are needed. The Society of Anesthesia and Sleep Medicine along with the Society for Obstetric Anesthesia and Perinatology have brought together a multidisciplinary team of anesthesia professionals, sleep medicine specialists, research scientists, maternal fetal medicine specialists, and a research librarian to review available evidence and offer recommendations for screening, diagnosis, and treatment for patients with OSA during pregnancy. I will include a link to the full guidelines which were published in Obstetrics and Gynaecology in August 2023.
Let’s go through some of these recommendations now. For screening, it is not recommended to screen all pregnant patients for OSA, but screening is recommended for the following people: BMI greater than 30, hypertensive disorders of pregnancy, and or gestational diabetes in the index or prior pregnancy. This screening should be performed between 6-29 weeks gestation. It is recommended to use a screening tool that has been validated in pregnant patients. You may want to consider using the pregnancy-specific OSA screening criteria proposed by Facco and colleagues or the BATE model, but the BATE model requires clinical training and further validation. Are you screening pregnant patients at your institution and if so, what tool are you using?
For diagnosing OSA in pregnant patients, it is important to consider home sleep tests when appropriate and to consider repeat postpartum testing since there are dynamic airway changes that occur during and after pregnancy. For treatment recommendations, the guidelines highlight the lack of evidence for OSA treatment leading to improved pregnancy-specific outcomes, but it is important to treat symptoms, modify objective outcomes of OSA, and to improve quality of life. These are the first guidelines to address specific considerations for OSA management in pregnant patients and we hope that you will check it out. See the link in the show notes.
We are so excited to have comprehensive guidelines for surgical and pregnant patients with obstructive sleep apnea throughout the perioperative period and pregnancy so that we can provide safe anesthesia care and work to improve outcomes in anesthesia and sleep medicine.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
Have you thought about joining the Society of Anesthesia and Sleep Medicine? I will include a link to the website in the show notes. This is a new and growing organization dedicated to advancing the science of sleep and sleep-disordered breathing and the interactions with anesthesia with the added benefit of working to improve clinical outcomes for patients with sleep-disordered breathing undergoing anesthesia care. There are many opportunities for you to join in with an individual membership and make a difference or better yet, sign up your whole department with a department membership.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2024, The Anesthesia Patient Safety Foundation
