Episode #212 Comprehensive Approaches to Pediatric Patients with Sickle Cell Disease and Workplace Violence Prevention
July 24, 2024
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
This is Part 2 of 2. Our featured article again today is from the June 2024 APSF Newsletter. It is “Preoperative Transfusion and Sickle Cell Disease in the Pediatric Patient” by Rahul Baijal, Priti Dalal, and Megha Kanjia.
Thank you to Rahul Baijal for contributing to the show today.
We hope that you will use these resources from the article during your preoperative planning.
Table 1: Preoperative Evaluation of the Child with SCD.16,17
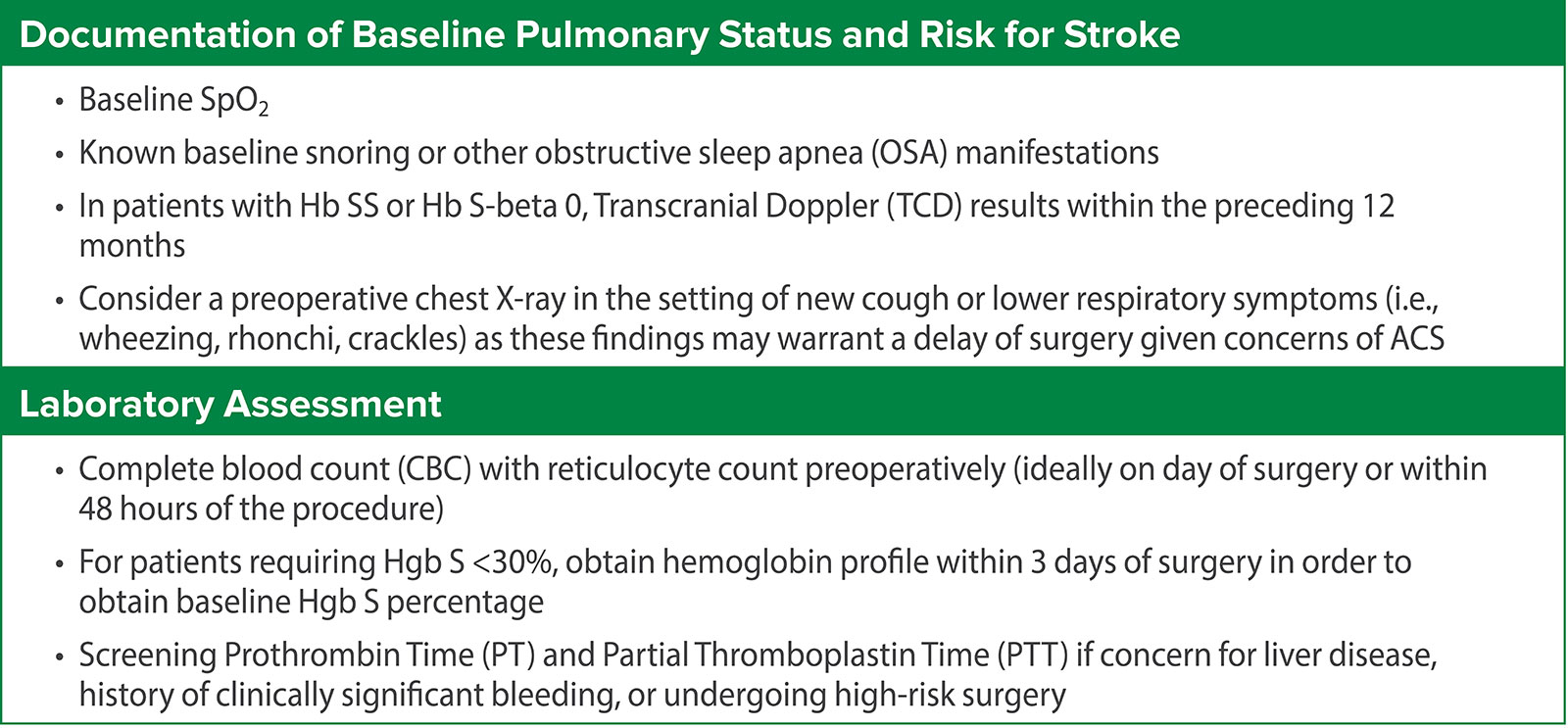
Table 2: Risk Stratification Based on Disease Severity and Type of Surgery.16,17
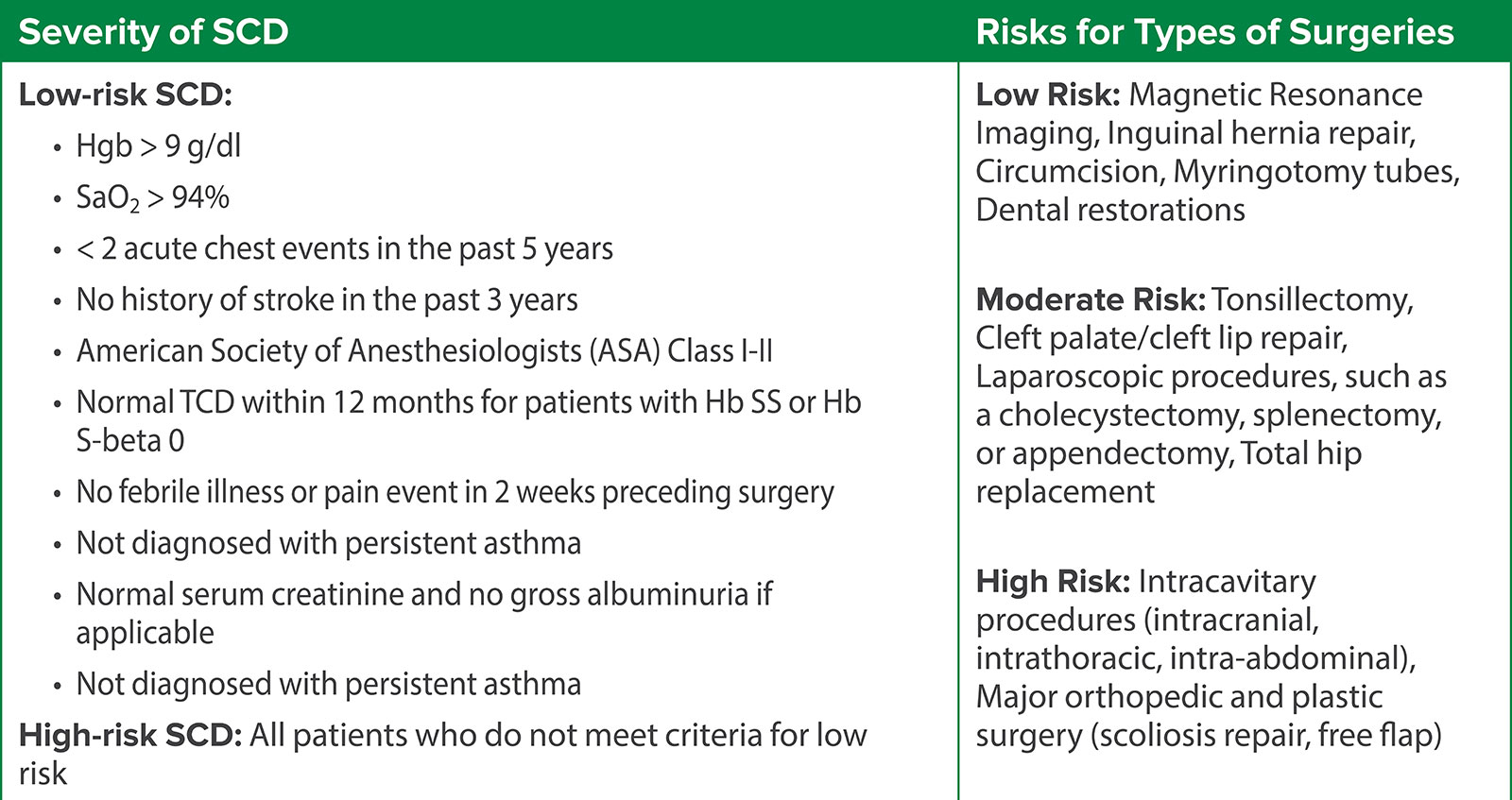
Table 3: Plan for Low-risk SCD.16,17
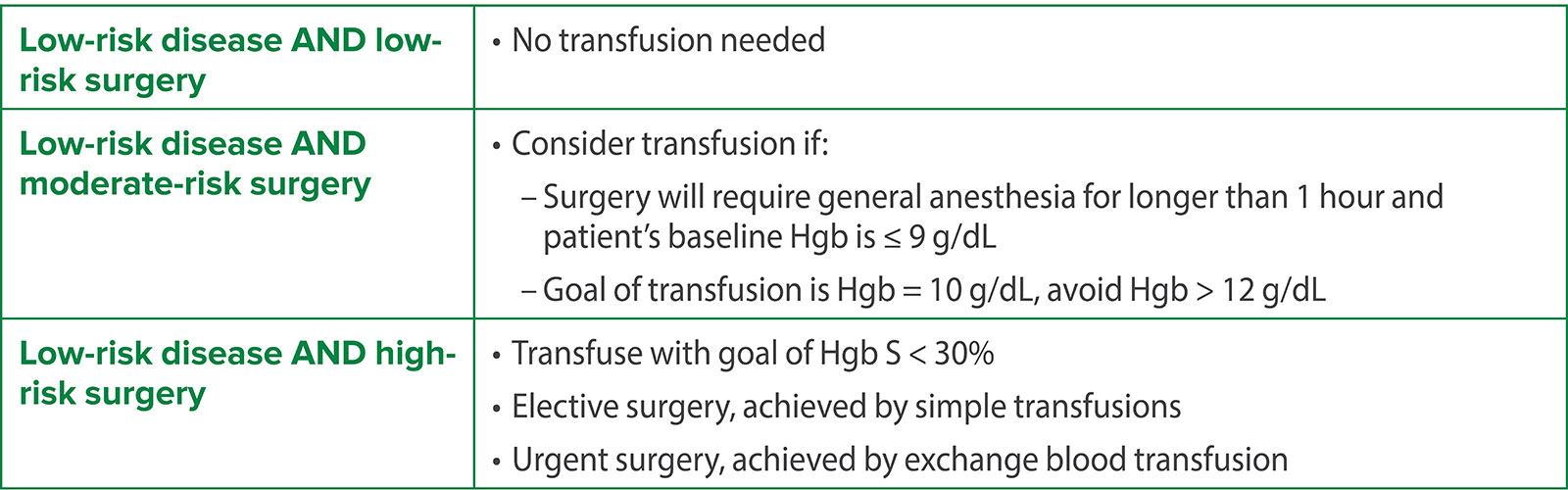
Table 4: Plan for High-risk SCD16,17
APSF is responding to the call to action to eliminate workplace violence.
We have created video-triggered workshop materials and tools designed to increase awareness, take perspective and stimulate conversation on responses within your workplace. The tools are ideal for integration into staff meetings, grand rounds, in-service training, and existing workplace violence curricula.
Please continue to return to this website as we add resources and use-case examples. Together we can eliminate workplace violence.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2024, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Our topic today is helping to keep pediatric patients with sickle cell disease safe during anesthesia care. We must remain vigilant to help prevent postoperative complications. Plus, pediatric patients with sickle cell disease have a different perioperative risk profile from adults with sickle cell disease. The development of a preoperative transfusion plan should be patient-specific with considerations for the sickle cell genotype, baseline hemoglobin, disease severity, risk classification of the surgery, and history of prior surgical complications.
Before we dive into the episode today, we’d like to recognize Medtronic, a major corporate supporter of APSF. Medtronic has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Medtronic – we wouldn’t be able to do all that we do without you!”
Our featured article again today is from the June 2024 APSF Newsletter. It is “Preoperative Transfusion and Sickle Cell Disease in the Pediatric Patient” by Rahul Baijal, Priti Dalal, and Megha Kanjia. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue and then scroll down until you get to our featured article today. I will include the link in the show notes as well.
Last week we reviewed sickle cell disease and did a literature review. Here are the highlights:
- Sickle Cell Disease occurs when there is a substitution of valine for glutamic acid on the beta chain of hemoglobin. Patients may be homozygous, Heterozygous, or have an associated thalassemia.
- Patients with sickle cell disease are at risk for sickle cell crisis during surgery and anesthesia if homeostasis is not maintained during the perioperative period. Remember, the triggers include hypothermia, hypoxemia, hypovolemia, infection, acidosis, pain, and stress which may occur during surgery and anesthesia care.
- Pediatric patients with sickle cell disease are at increased risk for postoperative complications including acute chest syndrome with an incidence of about 3%, stroke 0.2%, and 30-day mortality at 0.2%.
- Interventions that can help prevent sickle cell crisis include intravenous hydration, thermoregulation, and adequate oxygenation.
- There is controversy over appropriate preoperative transfusion strategies for patients with sickle cell disease.
- Guidelines from the American Society of Hematology in 2020 suggest transfusion to a hemoglobin level of 9 or 10g/dL in all patients with sickle cell disease undergoing surgery with general anesthesia that lasts for more than one hour.
- Routine preoperative blood transfusion in children with sickle cell disease is not recommended.
And that is where we are going to return to the article today. The authors highlight that the current literature on routine preoperative blood transfusion in children does not support this practice. This means that it is vital for an interdisciplinary team from anesthesiology, hematology, and surgery to work together to develop a patient-specific plan for preoperative transfusion with consideration for the following:
- The sickle cell disease genotype
- Baseline hemoglobin
- Disease severity
- Risk classification of surgery
- History of prior surgical complications
Let’s take a look at Table 1 from the article for an initial stepwise approach to the preoperative evaluation of a child with sickle cell disease. I will include this in the show notes as well.
First, it is important to document baseline pulmonary status and risk for stroke including the following considerations:
- Baseline SpO2
- Known baseline snoring or other obstructive sleep apnea manifestations.
- In patients with homozygous sickle cell or sickle cell beta thalassemia zero, transcranial doppler results within the preceding 12 months.
- Additional evaluation with preoperative chest Xray in the setting of a new cough or lower respiratory symptoms including wheezing, rhonchi, crackles) since these findings may be concerning for acute chest syndrome and a delay for the surgery may be needed.
The next preoperative step includes a laboratory assessment with the following:
- Complete blood count with reticulocyte count ideally on the day of surgery or within 48 hours of the procedure.
- For patients requiring Hgb S less than 30%, obtain hemoglobin profile within 3 days of surgery to get the baseline Hgb S percentage.
- You may also want to obtain a screening prothrombin time and partial thromboplastin time if there are concerns for liver disease, history of clinically significant bleeding, or it is a high-risk surgery.
We are moving on to Table 2 to help us make a decision for preoperative transfusion depending on the risk categorization based on the severity of sickle cell disease and type of surgery.
Let’s review risks for types of surgery.
Low risk surgeries include the following:
- Magnetic resonance imaging, inguinal hernia repair, circumcision, myringotomy tubes, dental restorations
Moderate risk surgeries include the following:
- Tonsillectomy, cleft palate/cleft lip repair, laparoscopic procedures such as cholecystectomy, splenectomy, or appendectomy, and total hip replacement
- High risk surgeries include the following:
- Intracranial, intrathoracic, and intra-abdominal procedures
- Major orthopedic and plastic surgery such as scoliosis repair or free flap reconstruction
The next step is to evaluate the sickle cell disease severity. Low risk disease includes the following characteristics:
- Hemoglobin greater than 9g/dL
- SaO2 greater than 94%
- Less than 2 acute chest events in the past 5 years
- No history of stroke in the past 3 years
- ASA Class I or II
- Normal transcranial doppler within 12 months for Hb SS or Hb S beta 0 patients
- No febrile illness or pain event in the 2 weeks before surgery
- No diagnosis of persistent asthma
- Normal serum creatinine and no gross albuminuria if applicable
High risk sickle cell patients are all of those who do not meet the criteria for low risk.
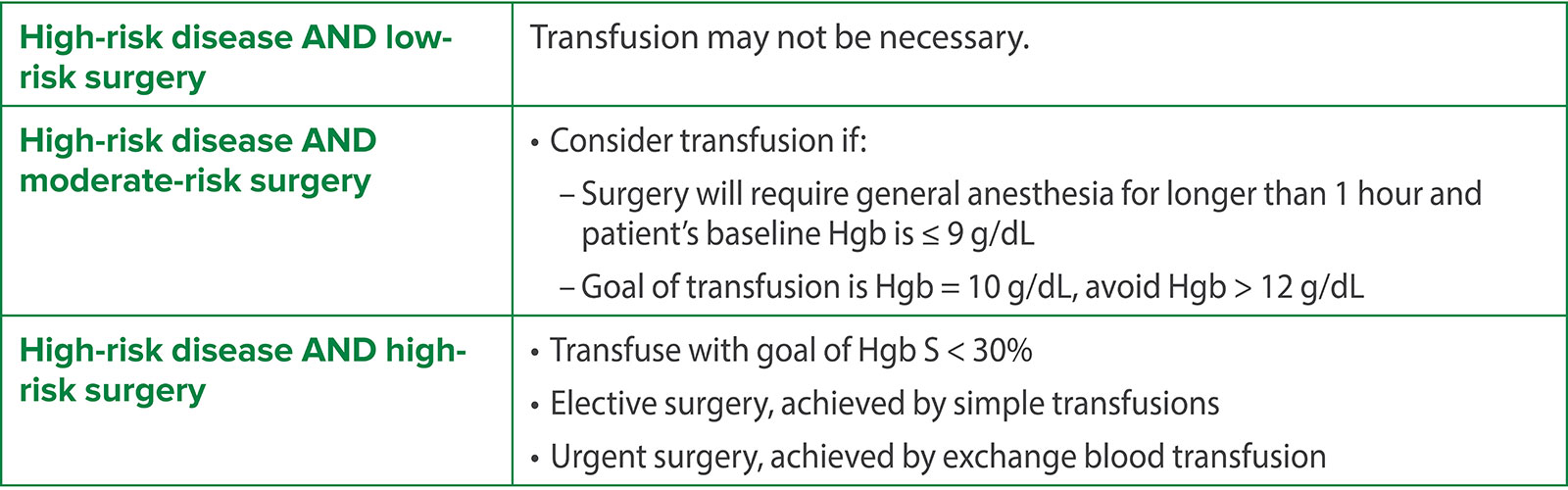
Let’s put it altogether into a plan. The authors provide a possible recommended plan based on the considerations that we just talked about for low risk and for high-risk sickle cell disease. These are included in table 3 and table 4 and we are going to review these plans now.
First up, here is the plan for patients with low-risk sickle cell disease depending on the surgical risk. For low-risk disease and low risk surgery, no transfusion is necessary. For low-risk disease and moderate risk surgery, consider transfusion if surgery requires general anesthesia for longer than 1 hour and the patient’s baseline hemoglobin is less than 9 g/dL. The goal for transfusion is Hgb level of 10g/dL with avoidance of hemoglobin levels greater than 12g/dL. For low-risk disease and high-risk surgery, transfuse with goal Hgb S less than 30% which may be accomplished for elective surgery with simple transfusion and for urgent surgery by exchange blood transfusion.
And now the plan for patients with high-risk sickle cell disease depending on the surgical risk. For patients with high-risk disease and low risk surgery, transfusion may not be necessary. For high-risk disease and moderate risk surgery, consider transfusion if surgery will require general anesthesia for longer than 1 hour and the patient’s baseline hemoglobin is less than 9 g/dL. The goal for transfusion is hemoglobin equal to 10g/dL with avoidance of hemoglobin levels greater than 12 g/dL. For high-risk disease and high-risk surgery, transfuse with goal Hgb S less than 30%. This may be accomplished with simple transfusion for elective surgery and with exchange blood transfusion for urgent surgery.
These tables are great resources for the preoperative evaluation and planning for pediatric patients with sickle cell disease. You can use them in your preoperative anesthesia clinic to assist with the interdisciplinary planning to help keep these patients safe during surgery and anesthesia care. The authors leave us with the call to action that the decision for preoperative transfusion for pediatric patients with sickle cell disease should be guided by disease severity and type of surgery. Transfusion is most likely to be beneficial for patients with high-risk sickle cell disease and those undergoing high-risk surgery. Going forward, research is needed to help develop guidelines and protocols to help clinicians who strive to provide safe and quality care for these high-risk patients.
Before we wrap up for today, we are going to hear from one of the authors. I will let him introduce himself now.
[Bajal] “Hello, my name is Rahul Bajal and I’m a pediatric anesthesiologist at Texas Children’s Hospital in Houston, Texas.”
[Bechtel] I asked Bajal what he envisions for the future with regard to the perioperative care of children with sickle cell disease. Let’s take a listen to what he had to say.
[Bajal] “Since children with sickle cell disease are at significant risk for perioperative complications, I would like to see consistent adoption of multidisciplinary guidelines for the care of these children.
Additionally, much of the evidence is not available. Surrounding perioperative blood transfusion and hydration therapy is retrospective. Well-designed prospective trials in children will provide further evidence in the care of these children.”
[Bechtel] Thank you so much to Bajal for contributing to the show today. We are looking forward to the future with adoption of multidisciplinary guidelines to help guide anesthesia professionals who care for pediatric patients with sickle cell disease.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
For more great resources related to anesthesia patient safety, we hope that you will head over to APSF.org and click on the Patient Safety Resources heading. One important resource is the video on Workplace Violence Prevention. Are you interested in stopping the toxic effects of healthcare workplace violence? Did you know that anesthesiology faculty had the largest proportions of reported harassment experiences in the past 12 months in 2022 in men 21.3% and women 52.6%. Plus, 71.6% of perioperative survey respondents of anesthesiologists, surgeons, CRNAs, CAAs, PACU nurses, and OR nurses report experiencing non-physical violence. The APSF is responding to the call to action to eliminate workplace violence. This resource includes video-triggered workshop materials and tools to increase your awareness, take perspective, and stimulate conversation on responses within your workplace. You can use these tools during staff meetings, grand rounds, in-service training, and existing workplace violence curricula. This is an important step towards eliminating workplace violence and an excellent resource that you can use at your institution.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2024, The Anesthesia Patient Safety Foundation
