Episode #201 Enhancing Regional Anesthesia Practices for Superior Patient Safety, Part 2
May 8, 2024
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
We are returning to the February 2024 APSF Newsletter and our featured article again today is “Safety Considerations in Peripheral Nerve Blocks” by Christina Ratto, Joseph Szokol, and Paul Lee.
We kick off the show today by reviewing the most recent version of the LAST Checklist.
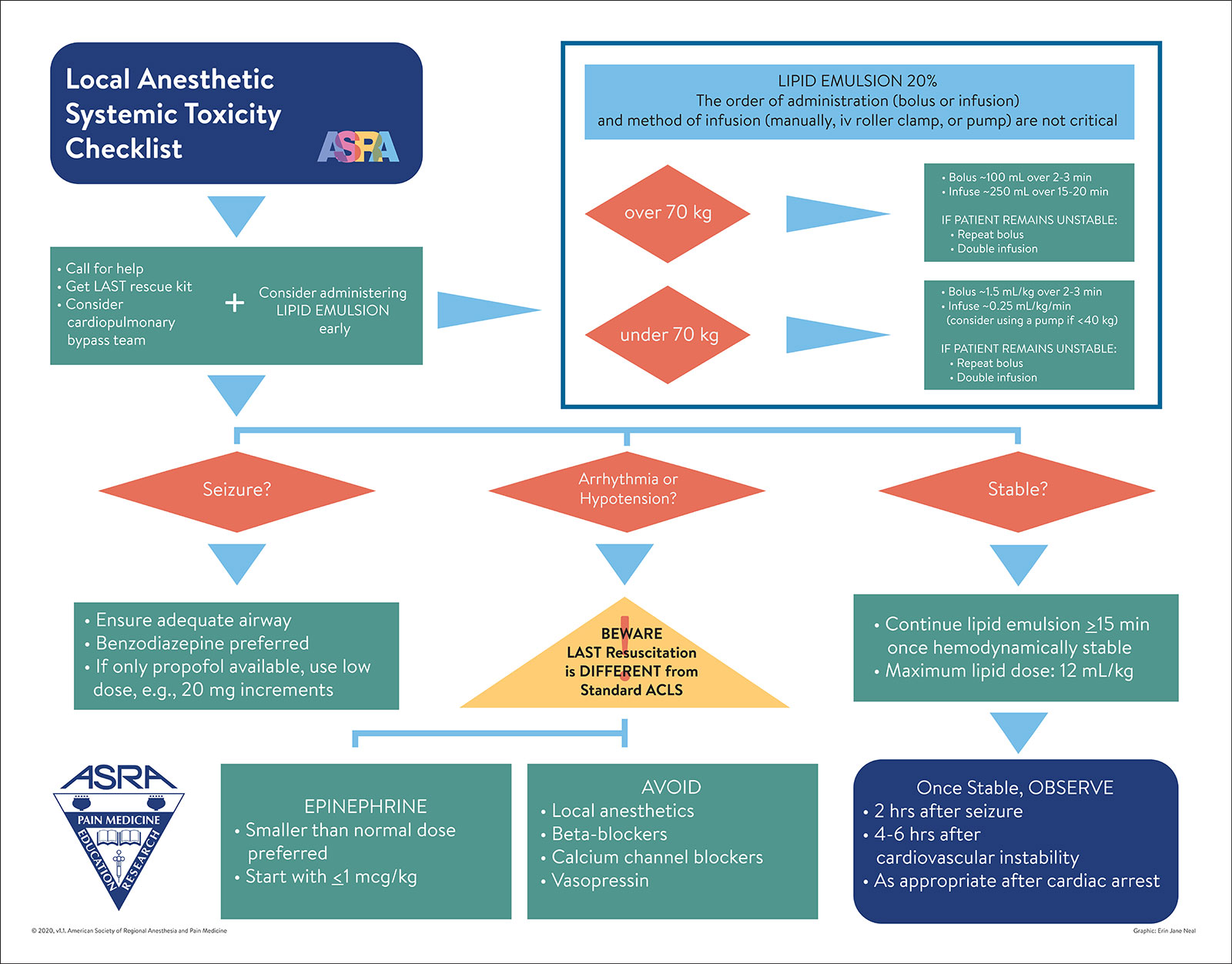
Figure 1. Local Anesthetic Systemic Toxicity Checklist.
Used with the permission of the American Society of Regional Anesthesia and Pain Medicine.
Here is the citation for the article that we reviewed on the show today.
- Taenzer AH, Walker BJ, Bosenberg AT, et al. Asleep versus awake: does it matter? Pediatric regional block complications by patient state: a report from the Pediatric Regional Anesthesia Network. Reg Anesth Pain Med.2014;39: 279–283. PMID: 24918334.
We also discuss the prevention of wrong-sided blocks. These are “Never Events” that occur at a rate of 7.5 per 10,000 procedures. Never Events are medical errors that should never happen as well as adverse events that are unambiguous, serious, and usually preventable. Check out Table 1 in the article for a list of factors that contribute to wrong-sided blocks. These factors include:
- Failure to verify site preoperatively
- Failure to mark area adequately by the surgeon
- Rushed, inadequate, or absent anesthesia timeout
- Distractions
- Patient position changes
- Scheduling changes
- Poor communication
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2024, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We are starting our next 200 episodes right now and continuing the conversation from last week all about anesthesia patient safety considerations and peripheral nerve blocks. So, make sure you have your ultrasound machine plugged in.
Before we dive into the episode today, we’d like to recognize Preferred Physicians Medical Risk Retention Group, a major corporate supporter of APSF. Preferred Physicians Medical Risk Retention Group has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Preferred Physicians Medical Risk Retention Group – we wouldn’t be able to do all that we do without you!”
We are returning to the February 2024 APSF Newsletter and our featured article again today is “Safety Considerations in Peripheral Nerve Blocks” by Christina Ratto, Joseph Szokol, and Paul Lee. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue. Then scroll down until you get to our featured article today. I will include a link in the show notes as well.
We have more exclusive content from Paul Lee, another author of the article. Here he is now.
[Paul Lee] Hi, my name is Paul Lee and I am the division chief of regional anesthesia and clinical assistant professor of anesthesiology at Keck Medical Center of the University of Southern California.”
[Bechtel] I asked Lee why he is interested in this topic. Let’s take a listen to what he had to say.
[Lee] “This topic has been an area of interest for me for many reasons. I’ve witnessed or reviewed multiple incidents during the timeout period prior to a block where the patient was at risk or harmed. Whether it’s a needle being injected into the wrong leg or application of antiseptic the patient was allergic to or a thoracic epidural being started even though the patient had just received heparin, many adverse events can be avoided by a simple reminder of safety surrounding neuraxial and peripheral nerve blocks.”
[Bechtel] Thank you so much to Lee for helping to kick off the show today. We are going to be hearing more from him so stay tuned! And now it’s time to get back into the article.
Our show ended last week by talking about the Local Anesthetic Systemic Toxicity Checklist. We are going to start by reviewing it now. I will include the checklist in the show notes as well. This is Figure 1 from the article.
Here are the first steps:
- Call for help
- Get LAST rescue kit
- Consider cardiopulmonary bypass team
- And with these three steps also consider early administration of Lipid Emulsion.
From here, we are going to review the lipid emulsion administration box. Keep in mind that the order of administration (bolus or infusion) and method of infusion (manually, IV roller, pump) are not critical.
- For over 70kg, bolus 100mls over 2-3 minutes and then 250mls over 15-20 minutes. If the patient remains unstable, repeat the bolus and double the infusion.
- For less than 70kgs, bolus 1.5 ml/kg over 2-3 minutes and then infusion 0.25ml/kg/min. Consider using a pump for patients who are less than 40kgs. If the patient remains unstable, then repeat the bolus and double the infusion.
Now, if we continue with the algorithm. If the patient has a seizure, the next steps are:
- Ensure adequate airway
- Benzodiazepine preferred
- If only Propofol is available, consider low dose of about 20mg increments.
If the patient has an arrhythmia or hypotension, remember that LAST resuscitation is different from standard ACLS.
- Make sure that you avoid local anesthetics, beta blockers, calcium channel blockers, and vasopressin.
- For epinephrine, a smaller than normal dose is preferred, so start with less than 1micogram per kg.
For patients who remain stable, continue lipid emulsion for more than 15 minutes after hemodynamic stability has been achieved. The maximum dose of lipid emulsion is 12ml/kg. Once stable, continue to monitor the patient for 2 hours after a seizure, 4-6 hours after cardiovascular instability, and as appropriate following a cardiac arrest.
Phew, we made it to the end of the checklist and that was a great review so that we are ready in case of a LAST event.
Do you perform your blocks on patients who are awake or under sedation or under general anesthesia? There is a case report published in 1998 of a thoracic epidural that was placed in a patient under general anesthesia. The patient suffered a spinal cord injury and permanent paraplegia after four attempts at epidural placement. What about peripheral nerve blocks though? There is not a lot of literature on the safety and risks of regional blocks in adults under general anesthesia. For pediatric patients, it is considered safe to perform regional blocks under general anesthesia. The Pediatric Regional Anesthesia Network is a multi-institutional research consortium which contains a registry of over 50,000 regional anesthetic blocks in pediatric patients under 18 years old. Check out the study, “Asleep versus awake: does it matter?: Pediatric regional block complications by patient state: a report from the Pediatric Regional Anesthesia Network.” I will include the citation in the show notes as well. The results reveal postoperative neurological symptoms under general anesthesia at a rate of 0.93 per 1,000 compared with 6.82 per 1,000 in sedated and awake patients with no cases of paralysis and only 1 case of a small sensory deficit in a sedated patient that lasted for more than 6 months. The authors of this study concluded that regional anesthetic blocks in pediatric patients under general anesthesia is as safe as in sedated or awake children. This was a prospective study that supports the prevailing standard of care in pediatric anesthesia for placing blocks in anesthetized patients. In adult patients, the more common practice is performance of regional blocks prior to induction of general anesthesia. It is likely that sedation may be beneficial to improve safety and success of the block with greater patient satisfaction. Going forward, we need more studies to evaluate the risk and benefit for regional anesthesia under general anesthesia in adult patients.
Next up, we are talking about prevention of wrong-sided blocks. These are “Never Events” that still occur, actually at a rate of 7.5 per 10,000 procedures. Let’s define Never Event. This is an egregious medical error that should never happen and was first introduced in 2001 by Ken Kizer, the former CEO of the National Quality Forum. The term also includes adverse events that are unambiguous, serious, and usually preventable. The first Never Event list was created in 2002 and now there are 7 categories with 29 “serious reportable events.” Check out Table 1 in the article for a list of factors that contribute to wrong-sided blocks. We are going to review the list now.
- Failure to verify site preoperatively
- Failure to mark area adequately by the surgeon
- Rushed, inadequate, or absent anesthesia timeout
- Distractions
- Patient position changes
- Scheduling changes
- Poor communication
There are important steps to take to help keep patients safe and avoid this big threat to anesthesia patient safety. Before starting your nerve block, make sure to perform a visual confirmation of the correct block location with the patient and nurse according to your institution-specific standards. Maybe that patient has a wristband marked with the word YES on the side corresponding to the surgery or a clear mark by the surgeon and anesthesiologist performing the procedure. It is important for the patient to participate in the process prior to administration of sedation or anesthesia to help decrease errors and improve patient satisfaction and patient safety. This transforms patients into active participants and helps improve confidence in the healthcare professionals taking care of them.
Another important consideration is for the anesthesia professional performing the block to discuss the operative procedure with the patient before providing anesthesia or sedation. The next step is for the patient to verbalize agreement with the correct procedure and surgical site with documentation of the discussion and patient verbalization on the consent form. Communication barriers for patients with sight and hearing impairments or non-English-speaking patients, or depending on emotional status need to be considered as well so that the patient can participate fully in the preoperative discussions with appropriate documentation in the medical record such as including the interpreter’s ID number. The responsibilities for the preprocedural nurse or procedural team include the following:
- Verify documentation such as the consent form, history of present illness and diagnostic data
- Identify any discrepancies or uncertainties
- Discuss these discrepancies with the surgical team prior to starting the procedure.
We are just about ready to perform the peripheral nerve block. The responsible anesthesia professional should use the “Universal Protocol” and take a preprocedural “Time out.” Check out Figure 2 in the article for a visual depiction of a Pre-procedure time out which should be performed immediately prior to incision or starting the nerve block. This needs to be performed in the same location as where the procedure will be performed, so if you are performing the block in the operating theatre, then the time out needs to be conducted in the operating theatre as well. The team members participating in the block need to be involved in the time out and this includes the anesthesia professional performing the block, the circulating nurse, and any other active participants who will be performing the procedure.
Let’s review the steps in the time out.
- First, confirm patient identity using two patient identifiers including name and date of birth
- Confirm agreement with the procedure that is to be done.
- Verify the correct side and site
- Verify the anticoagulation status and any allergies.
- Proceed with the block or procedure.
We made it to the end of the article. The authors highlight that regional anesthesia is a safe supplement or alternative to general anesthesia with benefits that include improved patient satisfaction and decreased opioid usage. Anesthesia professionals must ensure maximum safety while delivering excellent care. Important safety considerations include using ultrasound guidance when available, being able to recognize and provide treatment for LAST, and executing pre-procedural checklists to avoid the never event of a wrong-sided block.
Thank you to the authors for highlighting these important regional anesthesia patient safety considerations. Before we wrap up for today, we are going to hear from Lee again. I also asked him what is next for his research in this area. This is what he had to say.
[Lee] “My research largely centers most around regional anesthesia and enhanced recovery after surgery. Some of our upcoming projects include looking at utility of oral methadone and outpatient orthopedic surgeries and another project looking at the role of a PEX2 block for arthroscopic rotator cuff repairs.
My hope is that these projects will add to the expanding research in our community. further improving upon our surgical patient’s satisfaction.”
Thank you so much to Lee for contributing to the show today. We will stay tuned to learn more about these exciting projects going forward.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
The APSF Newsletter is published three times a year. We are still discussing the amazing February Newsletter articles and the next Newsletter release is fast approaching in June. There are also new articles published in between newsletter releases over at APSF.org. Have you read of these articles yet?
- The “APSF Workplace Violence Prevention: Video-Triggered Workshop”, published online on March 11, 2024
- An Article Between Issues, “Teamwork in the Operating Room: An Essential for Patient Safety” published on April 8, 2024
- And an In the Literature article, “A Dose-finding Study of Sugammadex for Reversal of Rocuronium in Cardiac Surgery Patients and Postoperative Monitoring for Recurrent Paralysis” published on April 15, 2024.
Head over to APSF.org and click on the Patient Safety Resources. Fourth one down is News and Updates. We hope that you will check it out.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2024, The Anesthesia Patient Safety Foundation
