Episode #200 Celebrating the 200th Episode – Safer Blocks and Enhancing Regional Anesthesia Safety
May 1, 2024
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
The Anesthesia Patient Safety Podcast has reached another huge milestone. This is our 200th episode!! We couldn’t have done it without all our listeners, the amazing APSF family, and the APSF NL authors who continue to highlight threats to safe anesthesia care and important considerations to help keep our patients safe. So go ahead and share some high fives!
To celebrate our 200th episode, we are turning on the ultrasound machine and drawing up some local anesthetic. That’s right, today’s show is all about peripheral nerve blocks and safe anesthesia care. Our featured article today is from the February 2024 APSF NL by Christina Ratto, Joseph Szokol, and Paul Lee. It is “Safety Considerations in Peripheral Nerve Blocks.”
Here are the citations from the articles that we talked about on the show today:
- Sites BD, MD, Taenzer AH, Herrick MD. Incidence of local anesthetic systemic toxicity and postoperative neurologic symptoms associated with 12,668 ultrasound-guided nerve blocks an analysis from a prospective clinical registry. Reg Anesth Pain Med.2012;37:478–482.
- Barrington MJ, Kluger R. Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade. Reg Anesth Pain Med. 2013; 38:289-99.
- Rosenblatt MA, Abel M, Fischer GW, et al. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Anesthesiology. 2006;105:217–218.
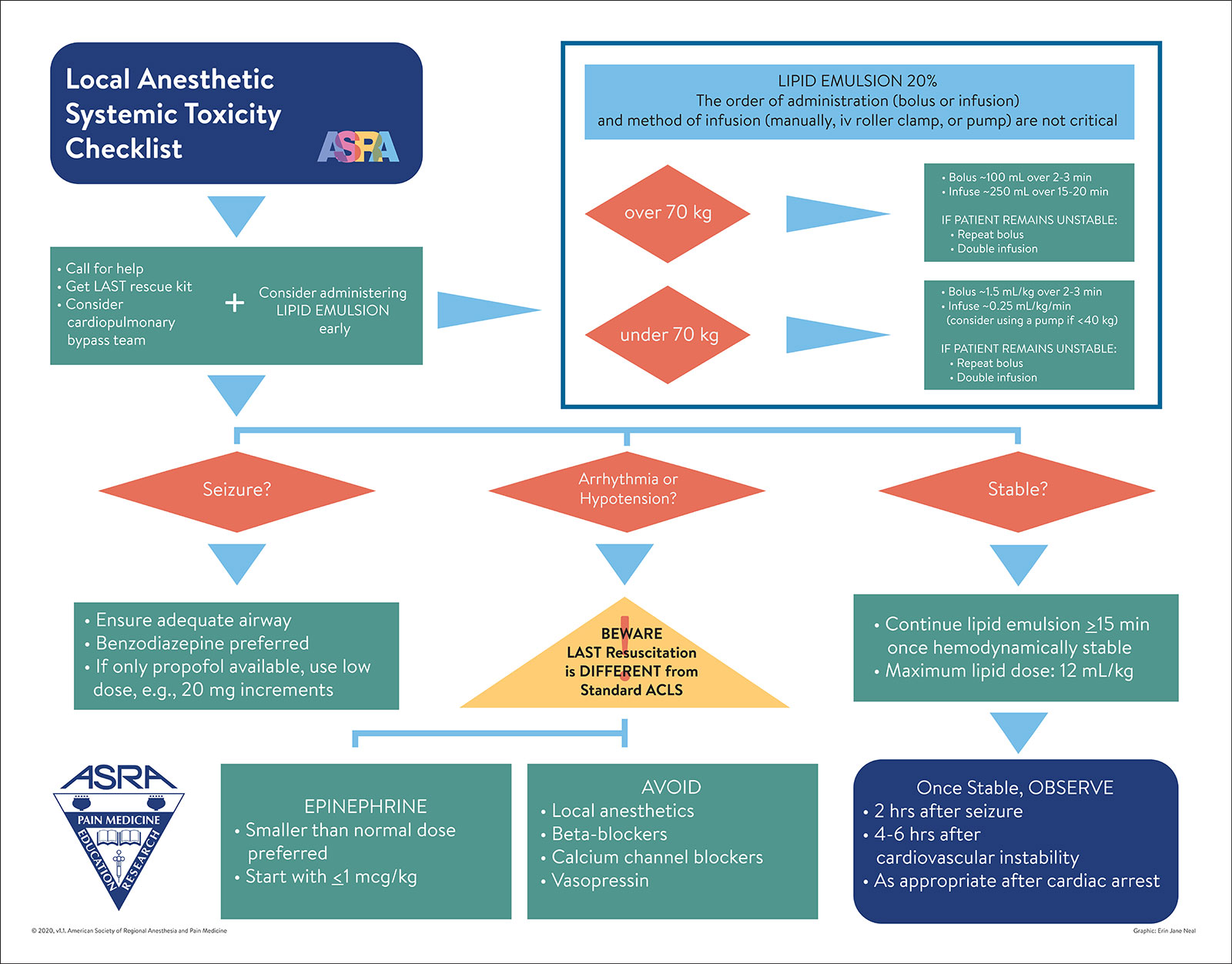
Figure 1. Local Anesthetic Systemic Toxicity Checklist.
Used with the permission of the American Society of Regional Anesthesia and Pain Medicine.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2024, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. And this is a very special show. The Anesthesia Patient Safety Podcast has reached another huge milestone. This is our 200th episode!! We couldn’t have done it without all our listeners, the amazing APSF family, and the APSF NL authors who continue to highlight threats to safe anesthesia care and important considerations to help keep our patients safe. So go ahead and share some high fives! To celebrate our 200th episode, we are turning on the ultrasound machine and drawing up some local anesthetic. That’s right, today’s show is all about peripheral nerve blocks and safe anesthesia care.
Before we dive into the episode today, we’d like to recognize Medtronic, a major corporate supporter of APSF. Medtronic has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Medtronic – we wouldn’t be able to do all that we do without you!”
Our featured article today is from the February 2024 APSF NL by Christina Ratto, Joseph Szokol, and Paul Lee. It is “Safety Considerations in Peripheral Nerve Blocks.” To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue. Then scroll down until you get to our featured article today. I will include a link in the show notes as well.
To help kick off our 200th episode today, we have one of the authors from the article. Here she is now.
[Ratto] “Hi, my name is Christina Ratto and I’m an anesthesiologist at Keck Hospital of USC in Los Angeles.”
[Bechtel] I asked Ratto why she is so passionate about this topic. This is what she had to say.
[Ratto] “I’m very passionate about regional anesthesia for both personal and societal reasons. On a personal level, I get tons of satisfaction in alleviating patients’ pain through these techniques. But I also value safety above all, and I believe it’s important to prioritize safe practices in all aspects of healthcare and this includes regional anesthesia. for your time. On a broader scale, I believe regional techniques can address important societal issues such as the opioid epidemic and substance abuse. I’m constantly advocating for regional anesthesia because the pain control is far superior, and the consequences of decreased opioids has far reached effects. And since we’re talking about patient safety, limiting opioids is another example of safer practices.”
[Bechtel] Thank you so much to Ratto for contributing to the show today. Don’t worry we will be hearing from Ratto again at the end of the show.
And now it’s time to turn on the ultrasound machine and get into the article. Here’s a brief overview of peripheral nerve blocks which are safe and effective alternatives or supplements to general anesthesia. These are handy tools in the anesthesia professionals’ toolbox to provide pain control during and after surgery while helping to avoid or decrease systemic opioids and the side effects. The benefits of peripheral nerve blocks include improved patient satisfaction, decreased resource utilization, and perhaps a better environmental footprint with decreased inhalational volatile gas administration. There has been a significant increase in the use of peripheral nerve blocks over time according to a study using the National Anesthesia Clinical Outcomes Registry data from almost 13 million outpatient surgeries between 2010 and 2015. Are peripheral nerve blocks part of your anesthesia practice? We are going to review safety concerns including nerve injury, recognition and treatment of local anesthetic systemic toxicity (LAST), and prevention of wrong-sided blocks with timeout protocols.
It is a good thing that our ultrasound is warmed up because we are going to start by talking about the role of the ultrasound during peripheral nerve blocks to improve patient safety. During your training, did you learn peripheral nerve stimulation technique or ultrasound-guided or a combination of the two? How do you practice now? Ultrasound-guidance has several benefits including improved block success, decreased need for rescue analgesia, decreased pain while performing the block, and lower rates of vascular and pleural puncture. For paravertebral and supraclavicular blocks, the use of ultrasound has not been shown to reduce the risk of pneumothorax in the literature, but visualization of the pleura while performing the block, may provide reassurance that the pleural space has not been punctured. We were optimistic that using ultrasound to directly visualize the needle and target nerve would further reduce the risk of nerve injury. But if we look at the literature, it does not reveal reduced postoperative neurologic symptoms with ultrasound-guided blocks compared to peripheral nerve stimulation. This post-block neurologic injury complication is likely due to mechanical injury to the fascicle and/or injection of local anesthetic into a fascicle causing myelin and axonal degeneration. The good news is that the neurologic symptoms are most often transient. Using data from the 3 largest registries, the incidence of long-term nerve injury following peripheral nerve block is 4 per 10,000 peripheral nerve blocks. This incidence is similar to the historic incidence before ultrasound was available and the blocks were performed with peripheral nerve stimulation technique. There may be factors related to the ultrasound equipment and the operator that can help to explain the current level of this devastating complication including the following:
- Quality of the ultrasound
- Skill of the proceduralist in identifying the intended nerve
- Inability to visualize the needle tip
- Misinterpretation of surrounding artifacts
- Needle movement and the use of hydro dissection does not prevent needle to nerve contact or vascular injection.
Let’s look at the study by Sites and colleagues, “Incidence of local anesthetic systemic toxicity and postoperative neurologic symptoms associated with 12,668 ultrasound-guided nerve blocks: an analysis from a prospective clinical registry” published in 2012. I will include the citation in the show notes as well. The investigators set out to determine the incidence of local anesthetic systemic toxicity and postoperative neurologic symptoms with ultrasound-guided peripheral nerve blocks. They used an 8-year time period and over 12,000 patients undergoing peripheral regional anesthesia to determine the incidence of postop neurologic symptoms, LAST, pneumothorax, and vascular trauma. Postoperative neurologic symptoms included any sensory or motor dysfunction that persisted for more than 5 days in a pattern consistent with the nerve block. The results are in for this study. The incidence of postoperative neurologic symptoms lasting more than 5 days was 1.8 per 1,000 blocks and this decreased to 0.9 per 1,000 blocks for symptoms lasting more than 6 months. Keep in mind that patients with preexisting neuropathy may be at increased risk for postoperative neurologic symptoms. It is vital to avoid intraneural injection to keep patients safe while performing peripheral nerve blocks.
The good news about ultrasound-guidance for peripheral nerve blocks is that it does significantly reduce the risk for another major complication, Local Anesthetic Systemic Toxicity. Check out the 2013 study by Barrington and Kluger, “Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade.” See the show notes for the citation. This study uses the Australian and New Zealand Registry of Regional Anaesthesia with 20 hospitals included over a 5-year time period from 2007 until 2012 to evaluate the occurrence of LAST following peripheral nerve block. Over 20,000 patients and over 25,000 blocks were included. The incidence of local anesthetic systemic toxicity was 0.87 per 1,000 blocks. Predictors of LAST included block site, local anesthetic used, dose per weight, total dose administered, and patient weight. Ultrasound-guidance helps to decrease the risk for LAST with real-time visualization of the needle and vessels to avoid vascular injury and intravascular injection of the local anesthetic. Another study determined that the incidence of LAST with ultrasound-guided blocks was incredibly low at 2.7 per 10,000 cases. Even with this minimal risk, it is important for anesthesia professionals to remain vigilant.
And speaking of LAST, we are moving on for a review and discussion of LAST. If we travel back to 1998, that is when we see the first case report of a potential treatment for LAST. Weinberg and colleagues used anesthetized rats and pre-treated with saline or different Intralipid solutions prior to administration of bupivacaine. In addition, saline or Intralipid was administered for resuscitation after bupivacaine bolus. The investigators found that the lipid emulsion could prevent, or reverse cardiac arrest caused by the bupivacaine overdose in the intact, anesthetized rat. The first successful use of 20% lipid infusion to resuscitate a patient following interscalene block with bupivacaine and mepivacaine who developed cardiac arrest was reported in 2006. Check out the Case Report published in Anesthesiology by Rosenblatt and colleagues. It is riveting. I am going to read some excerpts from it now and I will include the citation in the show notes as well.
“The patient was a 58-yr-old, 82-kg, 170-cm male who presented for arthroscopic repair of a torn rotator cuff in the right shoulder…. The patient arrived at the operating room holding area, where standard monitors were applied. Blood pressure was 120/80 mmHg, room air oxygen saturation measured by pulse oximetry was 98%, and heart rate was 60 beats/min. Supplemental oxygen was delivered at 3 l/min via a nasal cannula. A 20-gauge intravenous catheter was placed in the dorsum of his left hand, through which 2 mg midazolam and 50 μg fentanyl were administered. A 50-mm, 22-gauge Stimuplex® insulated needle was connected to a Stimuplex®-DIG nerve stimulator…and the interscalene groove was identified at the level of C6. The brachial plexus was identified by eliciting biceps stimulation … following which 40 ml local anesthetic solution (20 ml bupivacaine, 0.5%, and 20 ml mepivacaine, 1.5%) were injected slowly (over approximately 2.5 min) in 5-ml increments with gentle aspiration between doses. The patient was awake and conversant during the performance of the block. At no time was any blood aspirated, nor did he report pain or paresthesias.
Approximately 30 s after removal of the block needle, the patient became incoherent and then developed a tonic–clonic seizure. Oxygen was delivered by a facemask attached to a self-inflating resuscitation bag while 50 mg propofol was injected intravenously. The seizure stopped, and spontaneous respirations resumed. Approximately 90 s later, the patient began to seize again; this time, 100 mg intravenous propofol was administered. The electrocardiogram showed asystole, and no pulse, by carotid or femoral palpation, or blood pressure was detectable. Advanced cardiac life support was immediately started. The trachea was intubated, and end-tidal carbon dioxide was detected… During the first 20 min of advanced cardiac life support, a total of 3 mg epinephrine, given in divided doses, 2 mg atropine, 300 mg amiodarone, and 40 U arginine vasopressin were administered. In addition, monophasic defibrillation was used at escalating energy levels—200, 300, 360, and 360 J, according to the advanced cardiac life support protocol. The arrhythmias observed during most of the resuscitation period were pulseless ventricular tachycardia and asystole.
After 20 min, at which time plans were being made to institute cardiopulmonary bypass, the administration of a lipid emulsion was suggested, and 100 ml of 20% Intralipid (for Baxter Pharmaceuticals by Fresenius Kabi, Uppsala, Sweden) was given through the peripheral intravenous catheter. Cardiac compressions continued, and a defibrillation shock at 360 J was given. Within seconds, a single sinus beat appeared on the electrocardiogram, and 1 mg atropine and 1 mg epinephrine were administered. Within 15 s, while external chest compressions were continued, the cardiac rhythm returned to sinus at a rate of 90 beats/min. The blood pressure and pulse became detectable. An infusion of lipid emulsion was started and continued at 0.5 ml · kg−1· min−1over the following 2 h and then discontinued. The patient remained in sinus rhythm. He was weaned from mechanical ventilation, and his trachea was extubated, approximately 2.5 h later. He was awake and responsive and had right upper extremity weakness consistent with a brachial plexus block. No neurologic sequelae were sustained, and he was subsequently transferred to a monitored setting for overnight observation. There was no evidence of complications secondary to the administration of intralipid (i.e., pancreatitis) during the following 2 weeks.”
What an incredible case report and life-saving treatment with Intralipid.
The LAST checklist developed by the American Society of Regional Anesthesia and Pain Medicine was first published in 2010 and reviewed in 2012, 2017, and 2020. The most recent revision was in response to simulation and user feedback that earlier versions did not highlight the differences between LAST resuscitation and ACLS-guided resuscitation. This is critical and can be lifesaving since some of the standard medications used for ACLS including code dose epinephrine and vasopressin have been shown to worsen outcomes in LAST animal models. During simulation with the use of both LAST and ACLS checklists, there was confusion leading to delayed and wrong treatment during LAST resuscitation. The latest revision uses a standard triangular caution sign to highlight the differences between LAST and ACLS resuscitation. The dose for lipid emulsion has been simplified for patients over 70 kgs to receive a single bolus of 100mls followed by an infusion instead of needing to calculate an initial weight-based dose. Check out Figure 1 in the article to see the updated LAST Checklist and we will review this in more detail again next week. Before we wrap up for today, we are going to hear from Ratto again. I also asked her what she hopes to see going forward. Let’s take a listen to what she had to say.
[Ratto] “I envision a future where regional anesthesia is not only widely accepted, but it’s also the standard of care for a majority of surgical procedures.
There is so much versatility in the kinds of regional blocks we can offer. Everything from peripheral nerve blocks to truncal blocks. So, there’s really no limit to where we can provide pain control. We can do it anywhere in the body. Moving forward, we need to bring more attention to nerve blocks, their safe practices and their efficacy so that there’s widespread acceptance of them from everyone, including surgeons and patients.
I think as long as we keep this discussion open and continue to educate ourselves and each other, we will see further advances in this field, making it more and more safe, and also more and more common.”
[Bechtel] Thank you so much to Ratto for contributing to the show today. We are excited about further advances in the field of regional anesthesia and peripheral nerve blocks. We are also excited to continue to talk about this article next week for part 2. You don’t want to miss it when we continue the conversation about keeping patients safe during peripheral nerve blocks with considerations for performing these blocks under sedation and preventing wrong-sided blocks.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
Thank you for following along on this journey towards improved anesthesia patient safety for 200 episodes and counting. To celebrate, we hope that you will like, subscribe, share, and continue to download this podcast from wherever you get your podcasts. Thanks for listening.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2024, The Anesthesia Patient Safety Foundation
