Episode #185 Consensus Recommendations for Keeping Patients Safe During NORA Care, PART 1
January 17, 2024
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is from October 2023 APSF Newsletter. It is “Consensus Recommendations for the Safe Conduct of Nonoperating Room Anesthesia: A Meeting Report From the 2022 Stoelting Conference of the Anesthesia Patient Safety Foundation” by John Beard, Emily Methangkool, Shane Angus, Richard D. Urman, Daniel J. Cole.
Check out these links for the supplemental digital content for additional details and information about this process.
- Supplemental Digital Content 1, Table 1, http://links.lww.com/AA/E369
- Ethical considerations, inclusion and exclusion criteria, a list of speakers, and further details of the consensus development process can be found in Supplemental Digital Content 2, Appendix A, http://links.lww.com/AA/E370
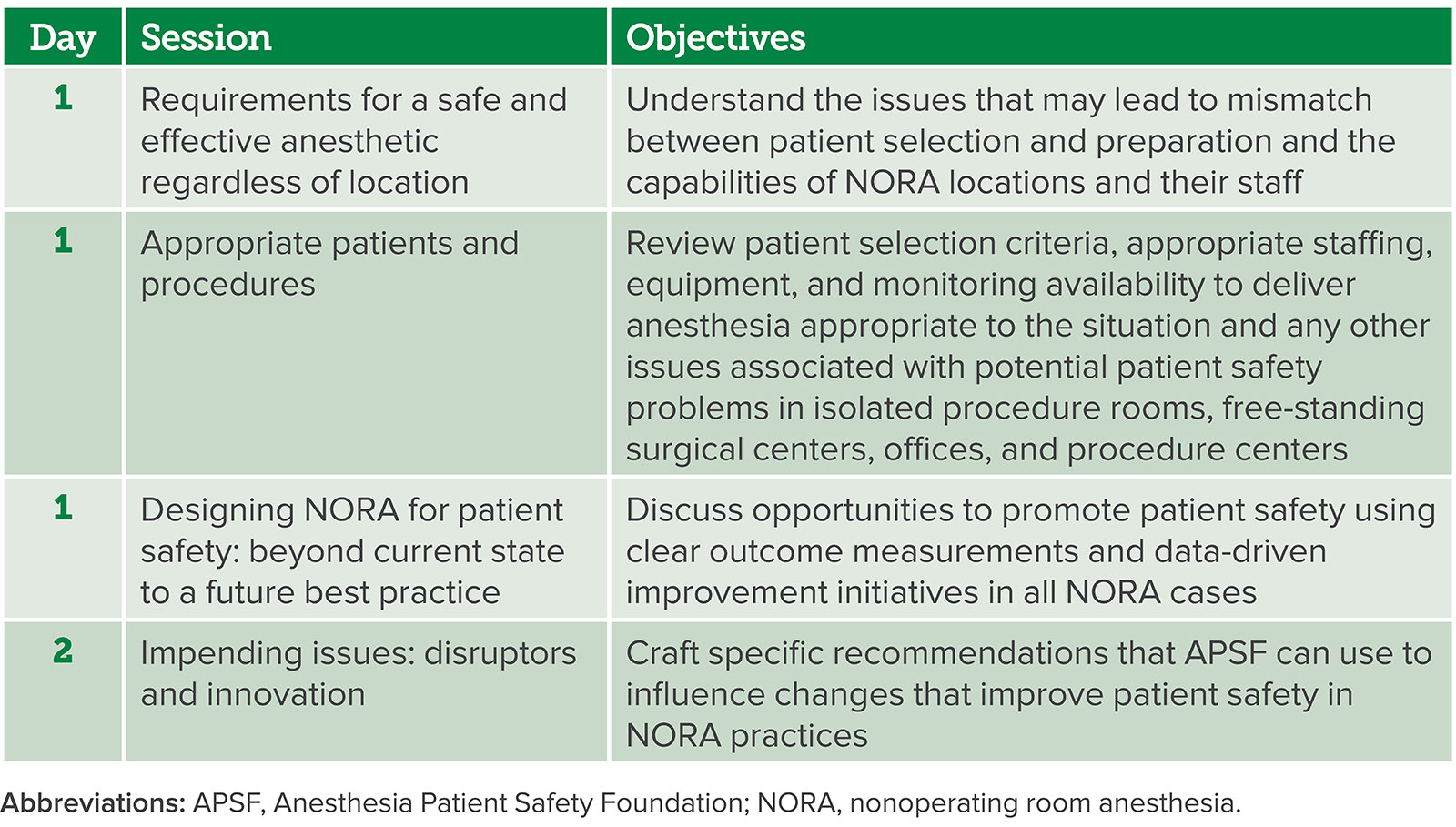
Table 1: 2022 Stoelting Conference Session Description.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2024, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Today, we are bringing you the latest in anesthesia patient safety recommendations related to Non-Operating Room Anesthesia, or NORA, Care. There are some important steps that we can take to help keep patients safe in NORA locations, so stay tuned.
Before we dive into the episode today, we’d like to recognize Edwards Lifesciences, a major corporate supporter of APSF. Edwards Lifesciences has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Edwards Lifesciences – we wouldn’t be able to do all that we do without you!”
Our featured article today is from October 2023 APSF Newsletter. You can also find this article in Anesthesia and Analgesia in August 2023. It is “Consensus Recommendations for the Safe Conduct of Nonoperating Room Anesthesia: A Meeting Report From the 2022 Stoelting Conference of the Anesthesia Patient Safety Foundation” by John Beard, Emily Methangkool, Shane Angus, Richard D. Urman, Daniel J. Cole. To follow along with us, head over to APSF.org and click on the Newsletter Heading. First one down is the current issue. From here, scroll down to our featured article today. I will include a link in the show notes as well. We have talked about keeping patients safe during NORA care on the podcast before. This was the focus of the 2022 APSF Stoelting Conference with the goal to create consensus recommendations for best practices in NORA pertaining to the following:
- Facility and location
- Equipment and supplies
- Staffing and teamwork
- Patient selection
- Periprocedural care
- Quality Improvement.
Today, we are going to hear from one of the authors of the article and review the recommendations. But first, we need to get to the NORA location.
[Footsteps walking clip]
Whew, we made it. Remember, NORA locations may be quite a distance away from the main operating theatres. Let’s hear from one of the authors now.
[Methangkool] “Hello, my name is Emily Methangkool and I’m the chair of the Department of Anesthesiology at all of you UCLA Medical Center.”
[Bechtel] To kick off the show today, I asked Methangkool why she feels so passionate about NORA. Let’s take a listen to what she had to say.
[Methangkool] “Providing anesthetic care outside of the operating room is particularly challenging given that these areas may be located far away from the main operating rooms. The rooms themselves may not be set up to accommodate anesthesia equipment, and the teams that work there may not necessarily be used to working with patients under anesthesia or with anesthesia professionals. There is evidence from closed claims data to suggest that patient safety issues, particularly with oxygenation and ventilation, are common in these areas and lead to patient harm. As anesthesia professionals, we have to ensure that we are providing the most optimal and safe care in these areas.
Thank you so much to Methangkool for helping to introduce this topic. Did you know that nonoperating room anesthesia or NORA cases are expected to be more than 50% of total anesthesia cases in the near future. These recommendations could not have come at a better time since there are challenges to providing safe anesthesia care including ergonomics, location, staffing, teamwork and communication, access to equipment, and lack of adequate preoperative optimization. Plus, I’m sure that you can think of more to add to this list. Evaluation of data from the American Society of Anesthesiologists Closed Claims database showed that adverse events occur in NORA locations at two times that rate of adverse events in the operating room. This is an excellent opportunity to improve anesthesia patient safety in NORA locations.
So, how did the APSF come up with these consensus recommendations? First, the conference planning committee which includes the authors of this article outlined the conference program and developed the first draft of NORA recommendations that was reviewed and revised by conference speakers and attendees with feedback during breakout sessions with a final presentation with time for discussion and voting. Following the conference, there were additional revisions with feedback from the conference planning committee, speakers, and participants. Check out the links in the article or in the show notes for the supplemental digital content for additional details and information about this process.
Here is an overview of the conference sessions and objectives:
- Requirements for a safe and effective anesthetic regardless of location with the objectives to understand the issues that may lead to mismatch between the patient selection and preparation and the capabilities of NORA locations and their staff.
- Appropriate patients and procedures with the objectives to review patient selection criteria, appropriate staffing, equipment, and monitoring availability to deliver anesthesia appropriate to the situation and any other issues associated with potential patient safety problems in isolated procedure rooms, free-standing surgical centers, offices, and procedure centers.
- Designing NORA for patient safety: Beyond current state to a future best practice with objectives to discuss opportunities to promote patient safety using clear outcome measurements and data-driven improvement initiatives in all NROA cases
- And the final session, Impending Issues: disruptors and innovation with the objectives to craft specific recommendations that the APSF can use to influence changes that can patient safety in NORA practices.
And now, it’s the moment you have all been waiting for, the recommendations. Here are the recommendations related to the facility.
- “Anesthesiology personnel should participate in planning, construction, expansion, or remodeling of NORA locations to ensure that patient safety and anesthetic needs are met.
- Anesthesiology personnel should encourage facility design teams to group NORA suites together, near the OR, or the PACU, to facilitate rapid access to additional personnel and equipment when needed.
- A reliable source of oxygen adequate for the length of the procedure and an immediately available backup supply are required. A central oxygen supply is ideal.
- A scavenging or capture system for anesthetic gas is required in locations where inhaled anesthesia is used.
- Electrical outlets shall be sufficient to supply anesthesia equipment and labeled to identify the backup power supply. The number of outlets available for backup power shall be sufficient to power equipment required to safely care for patients.
- Lighting shall be available to visualize the patient, equipment, supplies, and medications. Battery-powered backup lighting shall be available.
- There should be sufficient space to accommodate personnel with adequate clearance and expeditious access to the patient, equipment, supplies, and medications. Sufficient space shall be available to bring emergency equipment into the room.”
- A source of continuous suction shall be available and dedicated for use by anesthesiology personnel.
- Pre- and postprocedural areas shall be available for preparing and recovering the patient.
The next category is Equipment, Medications, and Supplies. Here are the recommendations:
- Anesthesiology personnel should participate in capital budget planning for equipment required to set up, maintain, and improve NORA services.
- When volatile anesthetics are administered, an anesthesia machine sufficient for case types and maintained to facility standards is required.
- Emergency airway equipment, including multiple forms of rescue (e.g., supraglottic airways, video laryngoscope, cricothyrotomy kit, etc.) is required for each NORA location.
- A self-inflating hand resuscitator bag capable of delivering positive pressure ventilation while administering at least 90 percent oxygen is required.
- In each NORA location, emergency supplies including a defibrillator, medications, and other equipment to provide cardiopulmonary resuscitation are required.
- Equipment and medication for treatment of MH shall be present in all locations where volatile anesthetics are used.
- Succinylcholine or other equivalent rapid acting paralytic medications should be immediately available for emergency airway management in all NORA locations. When succinylcholine is present, staff shall be educated on MH and prepared to provide and aid treatment.
- Infusion pumps should incorporate dose error reduction systems (DERS).
- Diagnostic testing capability appropriate for the patient population and planned procedures is required.
- Appropriate blood products and the equipment required for administration, such as a fluid warmer, shall be available for procedures that may have clinically significant blood loss.
- MRI-safe equipment, including airway equipment, infusion pumps, monitors, and anesthesia machines shall be available for MRI, and providers trained on their use. Patient monitoring consistent with operating room standards should be displayed in the MRI control room.
- Intralipid for treatment of local anesthetic systemic toxicity (LAST) shall be available at NORA locations where local anesthetic is used for purposes other than local skin infiltration.
- Patient size and weight capacity limits should be established for each NORA site to confirm patient suitability based on equipment and other available resources.
- Crisis manuals appropriate for the patient population, procedures, and potential therapeutic complications shall be available to staff and clearly visible in each NORA location to serve as cognitive aids during emergencies.
- Protective equipment, including, but not limited to lead aprons, goggles and radiation shields shall be made available to all anesthesia personnel where radiation exposure may occur.
- Equipment, such as inflatable mattresses, for patient transfer to and from procedure table shall be available to avoid injury to patient and personnel.
Next up, let’s review the recommendations for keeping patients safe in NORA related to staffing and teamwork. Here we go:
- “Communication, team building, expectations, and training should be established through a proactive collaborative process driven by anesthesiology personnel, nursing, surgical, and proceduralist leadership.
- In each NORA location adequate staff shall be trained to support the patient and the anesthesiology care team. The NORA team shall include at least two individuals with appropriate certification (ACLS, BLS, or PALS) and defined responsibilities to provide patient care during emergencies.
- Anesthesiology personnel should triage and evaluate complex cases, assist with scheduling, and optimize quality and safety protocols. A dedicated NORA anesthesiology team should be considered to facilitate communication and the adoption of protocols and pathways.
- Team members names and roles should be posted in the NORA location to facilitate communication during patient care.
The next category is Preprocedural care and patient selection. The following recommendations are related to these topics:
- A preprocedural evaluation process shall be established based on the ASA Practice Advisory for Pre-anesthesia Evaluation and emerging best practice.
- Adult and pediatric patient comorbidities should be identified which require specialized preoperative evaluation or necessitate procedural care in an inpatient facility.
- Adult and pediatric patients with elevated BMI or a diagnosis or suspected diagnosis of OSA should be evaluated on a case-by-case basis for suitability for the planned procedural location and management plan.
- Before each procedure, a timeout shall be conducted per The Joint Commission Universal Protocol or according to the facility protocol including site marking and laterality as indicated.
- Appropriate education shall be provided to team members for new or unfamiliar procedure types, and specific aspects of the case shall be reviewed with NORA staff.
- All patients should be assessed for fall and venous thromboembolism risk and treated appropriately.
Let’s get the procedure underway with the recommendations for intraprocedural care.
- Intra-procedural monitoring shall adhere to ASA Standards for Basic Anesthetic Monitoring with additional monitoring based on patient comorbidities and/or the nature of the procedure.
- A formal system to call for assistance, designate personnel to respond, and transport a patient with appropriate monitoring from the NORA location to an in-patient facility shall be established.
Once the procedure has been completed, here are the recommendations for post procedure care.
- Appropriate post anesthesia management shall be provided per ASA Standards for Post anesthesia Care.
- Recovery and discharge guidelines shall enable patient assessment in a simple, clear, and reproducible manner.
- Patients who receive medications for sedation or anesthesia (but not local anesthetics alone) shall be discharged with a responsible individual who can ensure the safe transport of the patient to their home.
In order to continue to make sure that patient safety is maintained in NORA locations, here are the recommendations for continuous quality improvement.
- Anesthesia personnel should establish a quality review process to identify possible new safety risks and improve care on a regular basis.
- Periodic emergency response simulations should be performed to review system, communication, equipment, and educational infrastructure.
We made it through all the recommendations! There is definitely a lot of work that can be done to improve anesthesia patient safety in NORA locations. Before we wrap up for today, we are going to hear from Methangkool again. I also asked her what she envisions for the future with regards to NORA care. Here is her response.
[Methangkool] “Actually, I hope that in the future we won’t even have to talk about NORA anymore…that it will just be a given that there will be the same standards of care, the same equipment and procedures and robust teamwork and communication in Nora so that we won’t even need to discuss patient safety issues in NORA any longer. How we get there is the actual question. And we do that by making sure that we are at the table and the C suite designing these areas and teams from the ground up and are at multidisciplinary hospital meetings to make sure that we reconfigure existing areas to ensure safety.”
[Bechtel] Thank you so much to Methangkool for contributing to the show today. With the help of these recommendations, we are looking forward to a future where we do not need to talk about the challenges of keeping patients safe in NORA locations. As we are working towards that goal, there is still more to talk about, so we hope you will join us for Part 2 next week.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
If you are enjoying listening to this podcast, and we hope that you are, we hope that you will also take a minute to subscribe, give us a 5-star rating, and leave us a review on iTunes or wherever you get your podcasts. We hope that you will share this podcast with your colleagues and team members, and anyone interested in anesthesia patient safety.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2024, The Anesthesia Patient Safety Foundation
