Episode #139 Understanding Cognitive Bias in Anesthesiology
February 28, 2023
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Today, we are talking about cognitive bias in anesthesiology. This is a threat to anesthesia patient safety so we need the tools to be able to recognize cognitive bias when it occurs, acknowledge the implications for patient safety, and work to reduce the impact of cognitive bias when we provide anesthesia care. Our featured article today is “Recognizing and Combating Cognitive Bias in Anesthesiology: Implications for Patient Safety” by George Tewfik, Stephen Rivoli, and Monica Harbell from the February 2023 APSF Newsletter.
What is the definition of cognitive bias? Check out this article for more background information.
- Landucci F, Lamperti M. A pandemic of cognitive bias. Intensive Care Med. 2021;47:636–637. PMID: 33108517
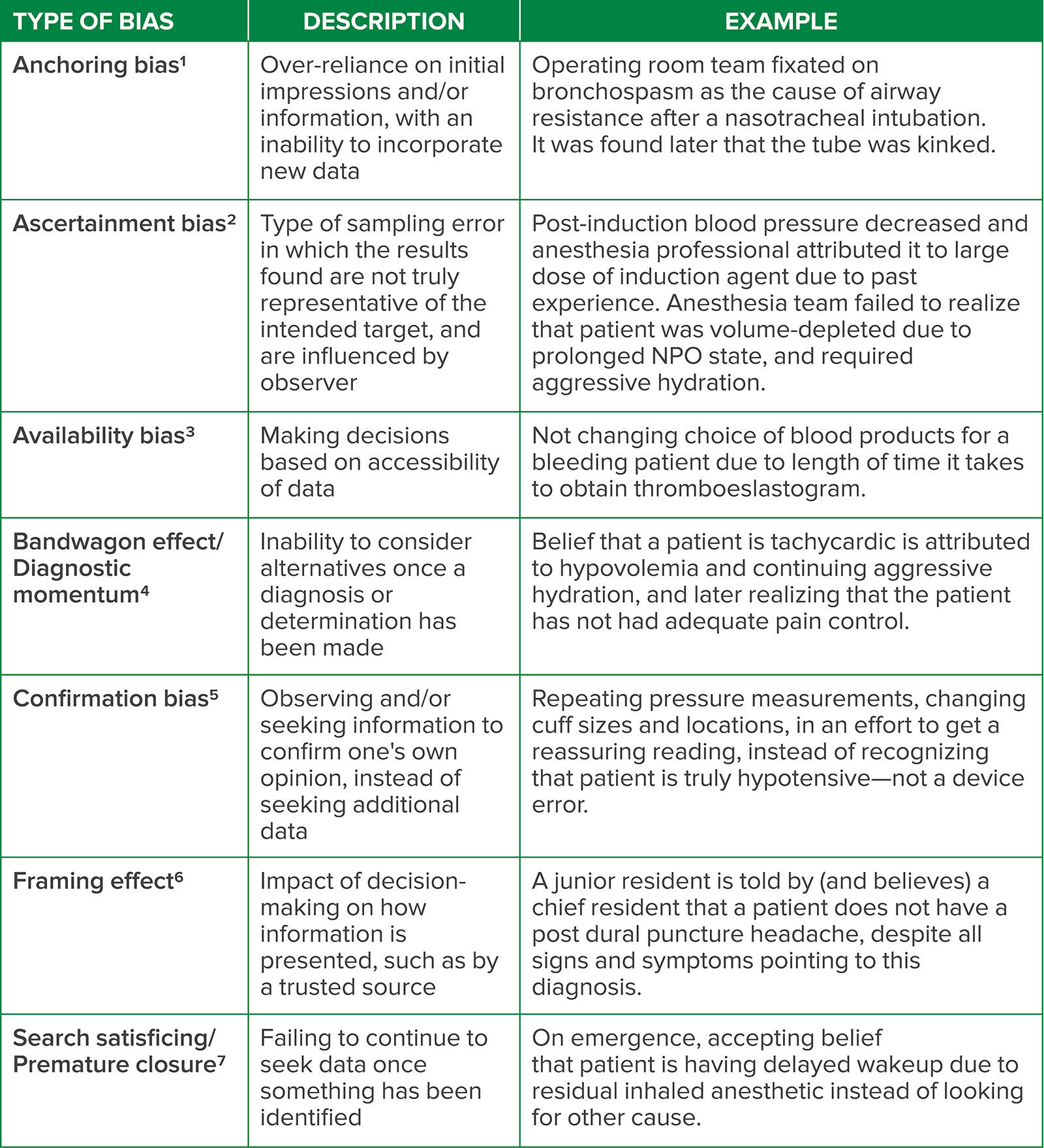
Table 1: A sampling of cognitive bias that may occur in anesthesiology and the practice of perioperative medicine, including descriptions and examples of each type.
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2023, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We are so excited about the release of the February 2023 APSF Newsletter. There are so many great articles. It was hard to decide which one to talk about first on the podcast, so I am just going to keep in you suspense a little longer…
But before we dive into the episode today, you’ve heard me recognize our corporate supporters on this show, but there’s another supporter who is absolutely essential – YOU! Every individual donation matters so much. Please visit APSF.org and click on the Our Donors heading and consider making a tax-deductible donation to the APSF.
Today, we are talking about cognitive bias in anesthesiology. This is a threat to anesthesia patient safety so we need the tools to be able to recognize cognitive bias when it occurs, acknowledge the implications for patient safety, and work to reduce the impact of cognitive bias when we provide anesthesia care. Our featured article today is “Recognizing and Combating Cognitive Bias in Anesthesiology: Implications for Patient Safety” by George Tewfik, Stephen Rivoli, and Monica Harbell from the February 2023 APSF Newsletter. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the Current Issue. From here, scroll down until you get to our featured article today. I will include a link in the show notes as well.
Now at this point, you may have some questions. What is cognitive bias? Have I ever been affected by cognitive bias? How do I recognize it? Let’s review the case scenario from the article for an opening example of cognitive bias during clinical anesthesia care. Here we go:
“After hearing the overhead page for emergency anesthesia help, an anesthesia professional rushed to the operating room with an Ear, Nose and Throat (ENT) case in progress. On arrival, she noted an asleep patient turned 90 degrees away from the anesthesia machine with an ENT laryngoscope in place with the following vital signs: 84% on the pulse oximeter and blood pressure 80/53 mmHg. She could hear the ventilator alarming, with “High Peak Inspiratory Pressure” flashing across the top of the screen. The anesthesia professional in the operating room at the time shared how the peak inspiratory pressures crept up quickly and ventilation was becoming difficult in the last several minutes. The patient had a history of asthma and despite bronchodilators and increased anesthetic, bronchospasm persisted. Another anesthesia professional auscultated and reported that there was no wheezing and no audible air movement; meanwhile, another colleague was preparing epinephrine. The anesthesia professional, who responded to the emergency anesthesia page, examined the patient from endotracheal tube to circuit to the machine and looked into the patient’s mouth where she saw the small endotracheal tube kinked out of sight from the anesthesia team. She relieved the bend and the ventilator alarm ceased its high-pitched whine. As the oxygen saturation quickly climbed, her colleagues’ faces showed both appreciation and embarrassment. How could they have missed that simple problem? The other emergency responders noted that they were so focused on assisting their colleague that they didn’t question the working diagnosis of bronchospasm. The in-operating room anesthesia professional noted that the history, timing, and signs led him to believe bronchospasm had to be what was happening. The second anesthesia professional, taking in new information without context, was able to correctly diagnose the problem. Unbeknownst to these anesthesia professionals, they were suffering from the effects of cognitive bias.”
Have you ever been in a case like this? Before we continue into the article, we are going to hear from one of the authors, Stephen Rivoli. Let’s take a listen now.
[Rivoli] “Hello, my name is Steven Oli. I’m an attending anesthesiologist and clinical assistant professor at NYU Langone in New York, New York.”
[Bechtel] To kick off the show today, I asked Rivoli what got him interested in this topic.
[Rivoli] “Well, my interest in this topic really came out of two separate things. First of all, my co-authors and I had presented at the ASA annual meeting several years in a row, a talk about adverse event analysis. And in that talk, we pay more than lip service to the idea that cognitive biases impact patient safety and are often a causal component of adverse events.
And around that same time, I experienced an event like in the vignette from my article, slightly less dramatic, but as the new eyes, as the person that came in and saw the event. I was struck by how pervasive cognitive biases can be, how insidious they can be, and moreover, how even strong clinicians can fall prey to them.”
[Bechtel] Thank you so much to Rivoli for contributing to the show today. Don’t worry, we are going to hear more from him later. Now, its time to get into the article. Here we go!
Let’s start with some background information. What is cognitive bias? This is when a clinician creates a subjective reality with the downstream effect of altered perception of a data point. Landucci and colleagues define cognitive bias as a “systemic pattern of deviation from an established norm or rationality in judgement” that may change practice and affect behavior. I will include the citation to their article, “A pandemic of cognitive bias” in the show notes as well. Keep in mind that cognitive bias occurs outside of medicine as well. In medicine, cognitive bias is a threat to patient safety for individuals and can lead to medical errors. Cognitive bias can also affect public health policy which may be a threat to health care on a larger scale as well.
The next step is to describe the different types of cognitive bias and understand the impact on patient safety. What types of cognitive bias were described in the case that we discussed that the beginning of the show? If you said availability bias and bandwagon effect, you are right. Take a look at Table 1 in the article for a list of cognitive bias that may occur while providing anesthesia care. We are going to review the descriptions and several examples now. I will include the Table in the show notes as well.
- Anchoring Bias involves the over-reliance on initial impressions and/or information with an inability to incorporate new data. Here’s an example: when the operating room team fixated on bronchospasm as the cause of airway resistance after nasotracheal intubation that was later found to be a kinked endotracheal tube.
- Ascertainment bias is a type of sampling error that occurs when the results found are not truly representative of the intended target, and are influenced by the observer. This bias may occur in the situation of post-induction hypotension that the anesthesia professional attributed to large bolus induction agent since this had happened in the past, but the anesthesia team did not recognize that the patient was volume-depleted due to prolonged NPO status and required an IVF bolus for treatment.
- Next up is availability bias which involves making decisions based on the accessibility of data. Here is an example: When the anesthesia professional taking care of a bleeding patient does not change the choice of blood products due to the length of time it takes to obtain results from a thromboelastogram.
- Bandwagon Effect which is otherwise known as diagnostic momentum and involves the inability to consider alternatives once a diagnosis or determination has been made. For example, when the anesthesia team believes that a patient is tachycardiac due to hypovolemia and provides continued aggressive fluid resuscitation, but then later realizes that the patient has not had adequate pain control.
- Confirmation bias occurs when observing and/or seeking information to confirm one’s own opinion instead of seeking additional data. Confirmation bias is at play when the anesthesia professional repeatedly checks the blood pressure, even changing the cuff size and location, in order to try to get a reassuring result, instead of recognizing that the patient is hypotensive and it is not a device error.
- Framing Effect is next. This bias involves an impact on decision-making based on how information is presented, such as by a trusted source. Here is the example: A junior resident is told by a chief resident that a patient does not have a post-dural puncture headache and the junior resident believes this is to be true despite all signs and symptoms pointing to this diagnosis.
- Search satisficing which is also known as premature closure involves failing to continue to seek data once something has been identified. For an example of this bias we can look at the following situation: on emergence, accepting the belief that the patient is having delayed wakeup due to residual inhaled anesthetic instead of looking for another cause.
Now that we have reviewed different types of cognitive bias and some examples, let’s discuss the effects of cognitive bias on errors during the perioperative period. Studies have shown that about 33% of all postoperative complications may be affected by bias and some of the specific types of cognitive bias are more likely to be a factor that impacts errors during anesthesia care. It is so important to be aware of cognitive bias and the effect on patient safety to help keep patients safe during anesthesia care. Let’s talk about confirmation bias and esophageal intubation. Remember, confirmation bias occurs when a person only observes or looks for information that confirms their current opinion instead of evaluating for more information that may challenge their current opinion. In the 2019 study, “Reducing the risk of confirmation bias in unrecognized esophageal intubation,” the authors reviewed a series of esophageal intubations that resulted in a catastrophic outcome for the patients. The results were that the anesthesia professional only used signs that confirmed their belief that a successful tracheal intubation such as thoracic movement, auscultation of the chest, fogging of the endotracheal tube, and perception of the tube passing the vocal cords instead of using the capnography tracing to confirm tube placement. This is confirmation bias at work in a clinical scenario that anesthesia professionals perform everyday.
Another way to evaluate the impact of cognitive bias in anesthesiology is to look at how different factors related to the healthcare professional, the patient, and systemic or external factors contribute to cognitive bias. Check out figure 2 in the article which we are going to review now. First up are the clinician factors that include cognitive load, fatigue, and personal considerations such as emotions. Next are the patient factors including complex patients with multiple comorbidities and incomplete information. The next category is systemic factors such as design of workflow, time considerations, information flow between providers, information technology, environmental limitations, poor communication, poor collaboration, and poor culture of support. Finally, we have the external factors of overconfidence, framing, personal preferences, emotions, feedback, shift of memory, anchoring, and loss aversion. These four categories contain many factors that may play a role in contributing to cognitive bias leading to errors during anesthesia care and threatening patient safety.
As you can see this is a very important topic. We hope that you will join us again next week as we talk about how to reduce cognitive bias in general and how to limit the impact of cognitive bias on patient safety during anesthesia care. Plus, we are going to hear from Rivoli again.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
If you have not done so already, we hope that you will rate us and leave a review on iTunes or wherever you get your podcasts and feel free to share this podcast with your friends and colleagues and anyone that you know who is interested in anesthesia patient safety.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2023, The Anesthesia Patient Safety Foundation
