Episode #123 A Guide to Infection Prevention for Anesthesia Professionals, Part 1
November 8, 2022
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is “A Best Practice for Anesthesia Work Area Infection Control Measures: What Are You Waiting For?” by Jonathan Charnin and colleagues. Plus, we have additional content from Jonathan Charmin on the show.
Check out this figure from the article. You can print it out and bring it to your next department meeting as a good starting point to make sure that you are able to implement these four features.
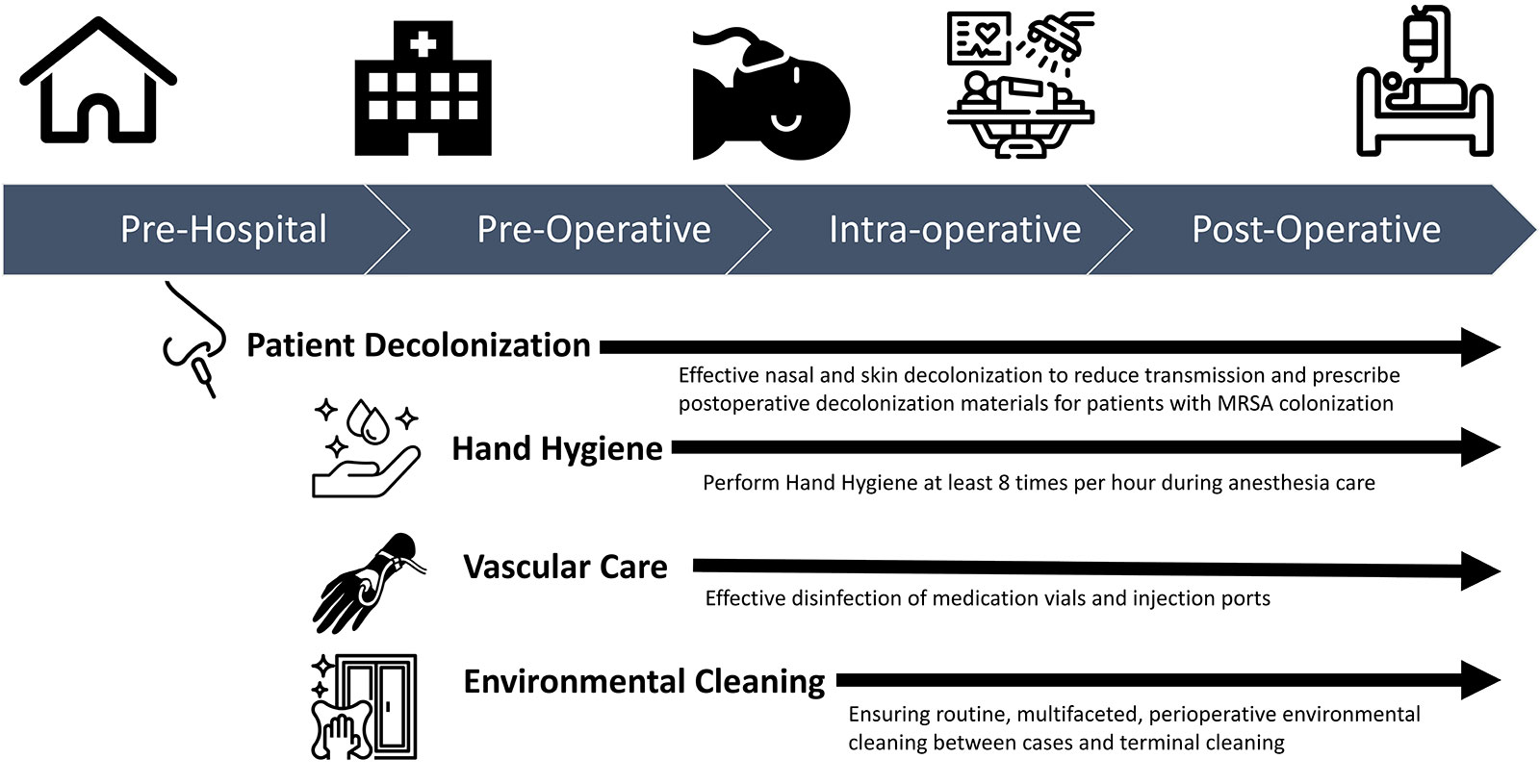
Figure 1: Evidence-based high-value opportunities to mitigate transmission of infection across the perioperative continuum.
We cover the first two measures today, patient decolonization and hand hygiene.
The recommendations for patient decolonization include the following:
- Two doses of 5% nasal povidone iodine within one hour of the surgical incision and use of 2% chlorhexidine gluconate wipes on the morning of surgery.
- An alternative strategy includes at least 2 days of treatment (ideally the day before and the day of surgery) with 5% nasal mupirocin ointment with 2% chlorhexidine gluconate wipes or 4% shampoo.
- Prescribe post-discharge decolonization for your patients colonized with methicillin-resistant Staphylococcus aureus (MRSA) as a result of the health care exposure.
The next intervention is Hand Hygiene which includes the following recommendations:
- Increase hand hygiene frequency during anesthesia care. Perform hand hygiene at least 8 times per hour during anesthesia care and at least 4 times per hour while providing care in critical care environments.
- Improve the frequency and quality of environmental cleaning to aid hand hygiene improvement efforts.
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2022, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. It may be November, but we are jumping back into the October 2022 APSF Newsletter. Today, we are heading to a space that is very familiar to anesthesia professionals, the Anesthesia Work Area which may be in the operating room or procedure room. Here we go.
Before we dive into the episode today, we’d like to recognize Merck, a major corporate supporter of APSF. Merck has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Merck – we wouldn’t be able to do all that we do without you!”
Our featured article today is “A Best Practice for Anesthesia Work Area Infection Control Measures: What Are You Waiting For?” by Jonathan Charnin and colleagues. To follow along with us, head over to APSF.org and click on the newsletter heading. First one down is the current issue. Then, scroll down until you get to our featured article today. Before we get into the article, we are going to hear from one of the authors. I will let him introduce himself now.
[Charnin] “Hi, my name is John Charnin and I’m an anesthesiologist and intensivist at Mayo Clinic in Rochester, Minnesota.”
[Bechtel] To kick off the show today, I asked Charnin why he wrote this article. Let’s take a listen to what he had to say.
[Charnin] “I joined a great team in writing this article because there’s already enough data for the anesthesia community to take action. We don’t need more studies to show us that these interventions are safe and effective. We just need to refocus the energy we learn to expand on Covid 19 mitigation and turn that towards a holistic approach to perioperative infection prevention. I hope this article helps to focus our efforts.”
[Bechtel] And with that, let’s focus our efforts and get into the article. Here is what we know and the scope of our topic today: there is evidence for basic infection control measures that may be used in the anesthesia work area that work to decrease pathogen transmission and surgical site infections. Infection is a big threat to patient safety. There is a call to action for anesthesia professionals to adopt these strategies to keep patients safe. Is this something that you are already doing at your institution? Is this something that you can help to implement at your institution? Keep listening as we discuss the preventive measures and the keys to successful implementation.
Infection prevention has skyrocketed to the top of considerations for patient safety in light of the emerging infectious diseases including Covid-19, Monkeypox, Candida Auris as well as persistent occurrence of surgical site infections and the associated increased patient morbidity and mortality. The authors remind us that any infection can lead to sepsis, so infection prevention is a vital step towards preventing sepsis. Anesthesia professionals must prioritize working towards improved patient safety using evidence-based strategies for infection prevention. These strategies are based on guidelines from the Society for Healthcare Epidemiology of America, Association for Professionals in Infection Control, Centers for Disease Control and Infection Prevention, American Society of Anesthesiologists, and the American Association of Nurse Anesthesiology. The good news is that these are simple, cost effective, practical strategies that revolve around the four pillars of perioperative infection control measures including patient decolonization, hand hygiene, vascular care, and environmental cleaning. We can polish these pillars with monitoring and feedback.
Let’s take a closer look at the possible routes for infection.
- Direct contamination of the wound
- Contiguous spread following patient skin contamination from existing colonization or colonization resulting from patient care
- Aerosolization of particles contaminated by pathogens arising from various anesthesia work area reservoirs which may include contaminated environmental surfaces and equipment
- Injection of bacterial pathogens from the injection port, syringe tip, and or medication vial contamination
As we talk more about these infection prevention strategies, think about your practice and your institution. Are you already using these measures? Have you considered all the implementation features? This is really important since single interventions without feedback optimization are unlikely to be successful. Check out Figure 1 in the article. This is a helpful infographic about perioperative infection prevention from before the patient even enters the hospital to the preoperative holding area, into the operating room, and all the way through the postoperative phase. You can find the figure in the show notes as well.
Now, it’s the moment you have been waiting for, Implementation of the Infection Prevention Measures. Here we go!
First up is Patient Decolonization. The recommendations include the following:
- Two doses of 5% nasal povidone iodine within one hour of the surgical incision and use of 2% chlorhexidine gluconate wipes on the morning of surgery.
- An alternative strategy includes at least 2 days of treatment (ideally the day before and the day of surgery) with 5% nasal mupirocin ointment with 2% chlorhexidine gluconate wipes or 4% shampoo.
- Prescribe post-discharge decolonization for your patients colonized with methicillin-resistant Staphylococcus aureus (MRSA) as a result of the health care exposure.
The authors provide the rationale for these recommendations. Staph aureus transmission occurs due to pathogen colonization of patient skin sites such as the nares, axilla, and/or groin and postoperative infection is often associated with this colonization. Thus, decolonization of these targeted skin sites is an important step towards decreasing surgical site infections. More research is needed to define the optimal timing for decolonization and something that we will be on the lookout for in the future. Patients who become colonized with MRSA in the hospital from health care exposure may benefit from postoperative decolonization which has been shown to decrease the development of an invasive infection for up to one year following the health care exposure. Keep in mind that prevention of MRSA transmission from health care exposure is an important consideration as well. The next part of this process is to work through the key implementation features. The decolonization agent is an important consideration taking into account increasing antibiotic resistance. Iodine and mupirocin are effective for surgical site infection prevention. Nasal mupirocin has been affected by increasing resistance, but that is not the case with iodine. Anesthesia professionals can manage preoperative iodine with two doses given prior to incision. Nasal mupirocin treatment is a longer course of 2-5 days preoperatively. Monitoring for patient and provider compliance with the decolonization prescription (either iodine or nasal mupirocin) is vital to ensure patient decolonization which may involve monitoring the utilization of decolonization supplies and providing feedback to the healthcare professional responsible for preoperative decolonization.
[Water Running Sound Effect]
The next intervention is Hand Hygiene which includes the following recommendations:
- Increase hand hygiene frequency during anesthesia care. Perform hand hygiene at least 8 times per hour during anesthesia care and at least 4 times per hour while providing care in critical care environments.
- Improve the frequency and quality of environmental cleaning to aid hand hygiene improvement efforts.
That is a lot of hand hygiene during a day of providing anesthesia care. Let’s review the rationale for these recommendations. As anesthesia professionals know, providing anesthesia care is fast paced with frequent interaction between the operating room environment, equipment, and the patient. There is a direct link between hand and environmental reservoirs which means that hand hygiene can decrease the risk for environmental infectious transmission. So, when should hand hygiene occur? The world health organization developed the “5 Moments of Hand Hygiene” which includes Before and after patient contact, after bodily fluid exposure, after contact with the contaminated environment and before performing a clean task. During a busy day in the operating theatre, it may be difficult to remember all of these moments. The principle of frequent and thoughtful hand hygiene is vital and easier to remember. There is a call to action for anesthesia professionals to do more to decrease the transmission of pathogens in the operating theatre. There is evidence for performing hand hygiene at least 8 times every hour to have a big impact on infection prevention. At the same time, it is important to maintain frequent and high-quality environmental cleaning which can further decrease infectious transmission from hand contamination. Donning double gloves for induction has been studied in simulated environments, but additional clinical research is needed.
What are the key implementation features of this measure? Hand sanitizers need to be positioned within easy reach of the anesthesia professional in the operating room which may require several places around the anesthesia work area. Alcohol-based Hand sanitizer locations may include on the anesthesia machine, mounted to the IV pole, on the providers waist. Keep in mind that hand hygiene is necessary for all members of the anesthesia team and all healthcare professionals on the perioperative team including circulating nurses, scrub technologists, surgeons, clinical anesthesia technologists, trainees, students, and equipment representatives. Anesthesia professionals may need to be leaders for hand hygiene implementation in the operating room, leading by example, strategies for positioning hand sanitizers, and with further education.
We still have two more infection prevention interventions to review all about vascular care and environmental cleaning, but you will have to tune in next week for the exciting conclusion. Plus, we are going to hear from Charnin again, so don’t miss it!!
Thank you so much to Charnin for contributing to the show today and we are looking forward to hearing more from you next week. We hope that you will be able to use some of these considerations to help keep your patients safe from infection during anesthesia care going forward. If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
We are spreading the word about the APSF podcast, and we hope that you will share this podcast with anyone you know who is interested in anesthesia patient safety including your surgical and procedural colleagues, trainees and students, nurses, and hospital administrators. You can connect with us on twitter @APSForg and using the hashtag #APSFpodcast and go ahead and tag a friend. Plus, you can find us on Facebook, Instagram, and Linked in. We would love to hear from you as we work towards improved anesthesia patient safety.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2022, The Anesthesia Patient Safety Foundation
