The FDA’s 2025 Early Alert regarding air embolism risks associated with the WATCHMAN Access System used in left atrial appendage occlusion (LAAO) procedures highlights important concerns related to anesthetic technique for this procedure. Despite advances in minimally invasive cardiac interventions and a shift toward sedation, recent reports of catastrophic air embolism underscore physiologic vulnerabilities when negative intrathoracic pressures occur during spontaneous ventilation, particularly during transseptal procedures. The FDA identified over 120 serious injuries and 17 deaths linked to preventable air embolisms. Anesthesia professionals play a key role in mitigating these risks and promote safer practice in the expanding field of structural heart interventions.
The field of structural heart intervention continues to evolve rapidly. Procedures such as transcatheter aortic valve replacement, transcatheter edge-to-edge repair, and left atrial appendage occlusion are associated with shorter hospital stays as compared to similar procedures ten years ago, without an increase in complications or mortality.1 Similarly, the choice of anesthetic technique for structural heart interventions has evolved to monitored anesthesia care with mild or moderate sedation.2 The decision to use mild or moderate sedation over general anesthesia for these procedures may hinge on proceduralist experience or patient factors, but is also frequently driven by the availability of anesthesiology resources, operating room block times, or transesophageal echocardiography. While earlier studies suggested that sedation may be associated with a shorter hospital length of stay and lower mortality, more contemporary and larger studies have not found a significant benefit.3,4 Although evolving sedation approaches can reduce recovery time and resource use, they may also introduce unique physiologic and procedural safety risks—particularly when device design or procedural steps may introduce air directly into the heart chambers.
Left Atrial Appendage Occlusion (LAAO) is a procedure that seals off the left atrial appendage in patients with non-valvular atrial fibrillation who are unable to take long-term oral anticoagulants. While the stroke risk reduction from LAAO is comparable to warfarin in major trials, the all-cause risk of stroke/systemic embolism and death at six months after LAAO is 1.2% and 4.0%, respectively.5,6 In August 2025, the U.S. Food and Drug Administration (FDA) issued an Early Alert highlighting a serious hazard with the access system for a LAAO device, the WATCHMAN.7 The alert reported multiple cases of catastrophic air embolism during WATCHMAN procedures performed under sedation with spontaneous ventilation and emphasized mitigation strategies to reduce the risk of air entrainment. For anesthesia professionals involved in these procedures, it is imperative to recognize and apply these strategies to prevent patient harm (Figure 1).
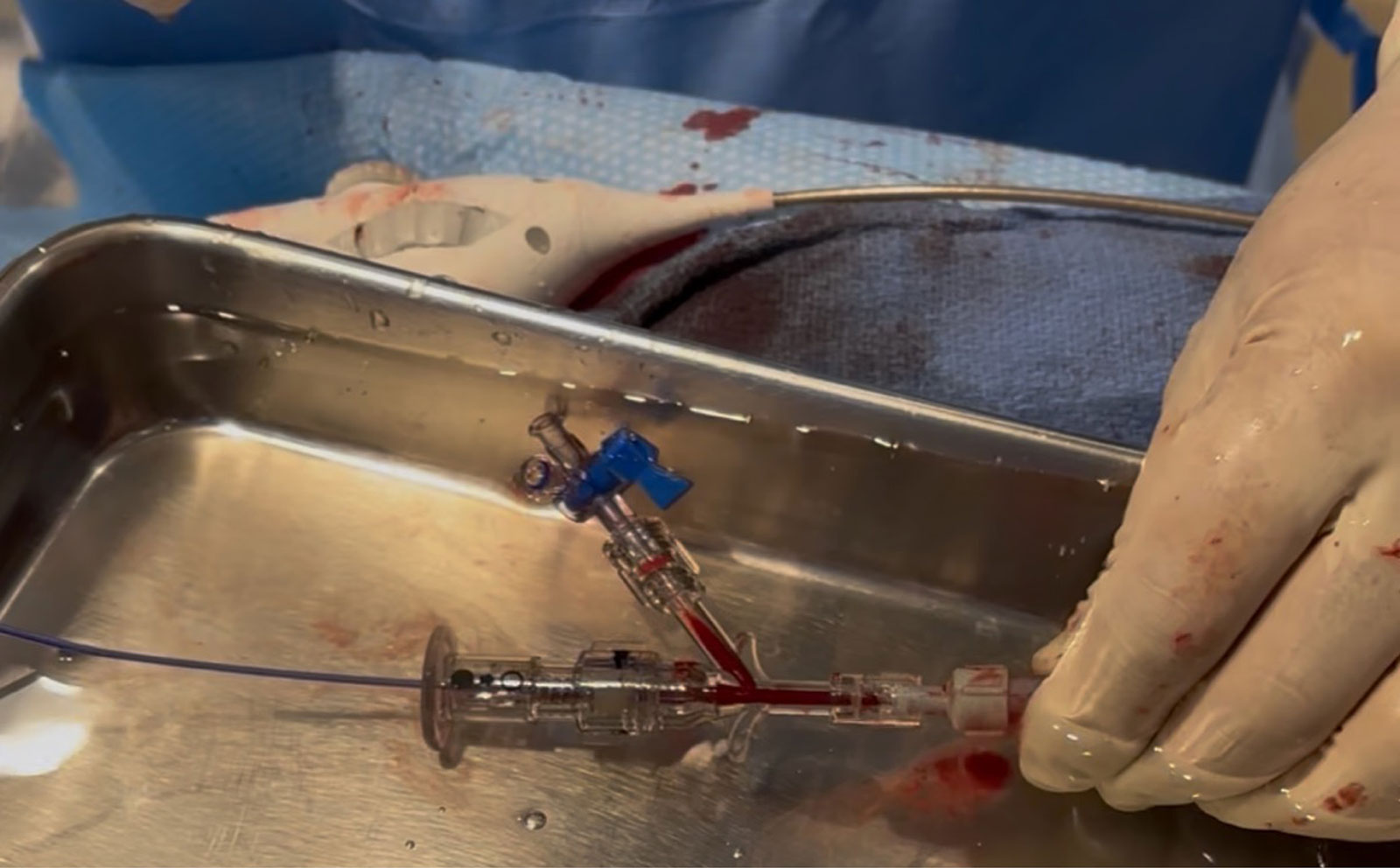
Figure 1: The proceduralist holds the delivery sheath connected to a Tuohy-Borst hemostatic valve with side-port stopcock. A pigtail catheter (left,} is coursing through the valve to access the left atrium. During device exchange, the connection is kept submerged under sterile water in a basin while the system is briefly disconnected to attach the Watchman delivery device.
THE FDA EARLY ALERT: KEY FINDINGS
The recent FDA and Boston Scientific safety communication reports 120 known cases of serious injuries and 17 deaths related to air embolisms during LAAO WATCHMAN procedures. The rates of air embolism during WATCHMAN procedures in a national registry (and reported to Boston Scientific) ranged between 0.03% and 0.06%.7,8 However, air embolism may go undetected because it is transient and may be clinically silent in sedated patients. For percutaneous heart procedures involving transseptal puncture to access the left atrium, a spontaneously ventilating, sedated patient has an approximately threefold increased risk of negative pressures in the left atrium and subsequent air entrainment.8 Identified risk factors for air entrainment into the heart during the procedure include spontaneous ventilation, upper airway collapse (obstructive sleep apnea), hypovolemia predisposing the patient to lower left atrial pressures, inadequate de-airing of the access system, and accidental injection of air. A recent study reported that even with the use of a non-invasive positive airway pressure device, over a third of deeply sedated patients undergoing transseptal puncture during sedation had inspiration-induced negative left atrial pressure (<0 mmHg) measured upon entry to the left atrium.9 The FDA alert warned that air could enter the LAAO access system during certain steps of device preparation or deployment, especially if the sheath or valve system was exposed to open air, inadequately de-aired, or positioned above the level of the heart during spontaneous ventilation.
The approach to LAAO using a delivery device involves transseptal puncture with a 14 French catheter.10 Entrainment of air through the device means that air directly enters the left atrium. Clinical sequelae of this include ST-segment changes due to coronary artery air embolism, hemodynamic instability and wall motion abnormalities, and air embolism to the brain resulting in stroke.
Transesophageal echocardiography can help monitor the catheter position and guide transseptal puncture when patients are under general anesthesia; however, the use of either transthoracic echocardiography or intracardiac echocardiography using a percutaneous catheter has become increasingly common for patients who are not intubated. The FDA provided various suggestions for risk mitigation strategies and precautionary measures (Table 1).7
Table 1: Precautionary Measures and Mitigation Strategies.
| Summary of precautionary measures and mitigation strategies to prevent air entrainment during minimally invasive heart procedures, especially those requiring transseptal puncture. | |
| Hemodynamic Optimization | Correct hypovolemia before puncture to prevent negative left atrial pressure and air entrainment. |
| Device Handling | Keep all sheaths, stopcocks, and access valves below the level of the heart and continuously filled with fluid. |
| De-Airing Technique | Ensure meticulous de-airing of all access systems, flush lines slowly, and maintain a continuous fluid column during device exchanges. |
| Exchange Protocol | Perform sheath or wire exchanges under saline or a water bath, withdraw devices slowly, and—if under spontaneous ventilation—make exchanges during expiration. |
| System Readiness | Verify that all air elimination and valve seals are confirmed before insertion; use clear communication between cardiology and anesthesia prior to each exchange. |
Table 2: Periprocedural Safety for Anesthesia Professionals
| List of safety principles for anesthesiology professionals involved in minimally invasive heart procedures with risk of air embolism. | |
| Ventilation Strategy | Consider controlled PPV for higher-risk patients (e.g., OSA) to avoid negative intrathoracic pressure; use PEEP as appropriate. |
| Monitoring and Awareness | Maintain situational awareness during sheath manipulation; monitor airway pressures, hemodynamics, and echocardiographic views (TEE or ICE). |
| Team Communication | Establish clear role assignments for sheath control, flushing, and line management before starting the procedure. |
| Immediate Response Preparedness | Be ready to recognize and treat air embolism: Trendelenburg positioning, hemodynamic support, aspiration if indicated, and activation of perfusion/circulatory support teams. |
| Continuous Improvement | Stay current with FDA alerts, registry data, and device updates; participate in multidisciplinary reviews and simulation of rare events. |
Abbreviations: positive-pressure ventilation (PPV), positive end expiratory pressure (PEEP), transesophageal echocardography (TEE), intracardiac echocardiography (ICE), Food and Drug Administration (FDA).
PHYSIOLOGIC RATIONALE AS TO WHY SEDATION MAY INCREASE RISK
Under spontaneous ventilation, negative intrathoracic pressure can generate a suction gradient that favors air entrainment into open or inadequately sealed vascular systems. Even small volumes of air introduced into the left atrium can result in life-threatening cerebral or coronary embolic events. In contrast, general anesthesia with positive-pressure ventilation maintains a protective “outward” pressure gradient that may reduce this risk. However, this benefit must be weighed against procedural and patient factors such as severe pulmonary hypertension, valvular disorders, heart failure, respiratory failure, or neuromuscular diseases. Awareness of the involved physiology and closed loop communication with the procedural teams are essential during a procedure involving transseptal access where the mode of ventilation alters the direction of pressure gradients across an “open” cardiac access system.
LESSONS FROM ELECTROPHYSIOLOGY LITERATURE ON TRANSSEPTAL PUNCTURE FOR CARDIAC PROCEDURES
Parallels to the challenges of LAAO procedures can be drawn from interventions performed in the electrophysiology (EP) lab. A common EP procedure that crosses the interatrial septum is pulmonary vein isolation for treatment of atrial fibrillation. Catheter ablation for pulmonary vein isolation can be performed with multiple energy sources using different catheters including cryoballoon ablation, radiofrequency ablation, or pulse field ablation. This is commonly done under general anesthesia, but there are centers that perform the procedure under sedation. A prospective multicenter study from an Israeli registry of 1002 patients comparing sedation vs general anesthesia showed no difference in neurologic events.11 A recent meta-analysis comparing recurrence of atrial tachyarrhythmias between sedation and general anesthesia found no difference in recurrence rate or overall complications.12
While the overall reported risk of air embolism in registries is low, there are some studies that report that atrial fibrillation ablation cases could have rates of air embolism as high as 1.5%.13 Air embolism can present as myocardial ischemia in the right coronary artery territory, given that its more anterior position in a supine patient increases the likelihood of air entry. Prior studies from the electrophysiology literature have shown air entrainment during both ablation and mapping catheter utilization. The factors contributing to the volume of air entrained included sheath/catheter size mismatch, catheter tip shape, and the design of the hemostatic valve.14 Pulse field ablation sheaths are now designed with clear shafts which has resulted in air bubbles being directly observed by operators, which is especially important given the larger sheath size required for ablation catheters.
Mitigation strategies include recommendations to monitor all infusion lines for bubbles and withdraw catheters slowly with simultaneous aspiration by an interventionalist.3 One study showed that an increase in the magnitude of negative pressure in the sheath led to an increase in air entrainment, which could be mitigated by using a sheath-in-sheath technique.15 This technique involves leaving a smaller inner sheath or dilator inside the transeptal sheath at all times during exchanges with a continuous saline drip, creating a continuous fluid-filled column to prevent air entry during catheter exchange. Other investigations of air embolism during radiofrequency ablation and cryoballoon ablation procedures found that embolisms and air entrainment were reduced by slow flushing of sheaths, temporary balloon inflation prior to insertion, or by carrying out sheath access under a water bath.16,17
SYSTEM-LEVEL OPPORTUNITIES
Although anesthesia professionals can use specific intraoperative management strategies to reduce device-related adverse events, system-level improvements are also necessary (Table 2). Establishing clear sedation versus general anesthesia criteria that account for patient and physiologic risk inherent to the procedure is imperative. Oversight and competency training may be required for procedural steps previously not utilized or the implementation of procedural checklists for de-airing and sheath positioning to improve reliability over time. Enabling health care professionals in the operating room to speak up about compliance with safety procedures is essential. Adverse outcomes or device failures should be reported to the FDA for all suspected device-related adverse events.
CONCLUSION
As minimally invasive heart interventions increase in number and scope, anesthesiology professionals remain uniquely positioned to identify physiologic and procedural hazards before patient harm occurs. Mitigating the serious risks reported with LAAO or heart procedures requiring transseptal puncture requires both system level action plans along with close collaboration between anesthesiology, nursing, and cardiology teams to promote safety in this evolving area of cardiovascular care.
Daniel McGrail, MD, is an assistant professor of anesthesiology and critical care at SSM Health Saint Louis University Hospital, Saint Louis, MO.
Furqaan Sadiq, MD, is an assistant professor of anesthesiology and critical care at SSM Health Saint Louis University Hospital, Saint Louis, MO.
Divya Ratan Verma, MD, is an associate professor of cardiology at SSM Health Saint Louis University Hospital, Saint Louis, MO.
Govind Rangrass, MD, FASA, is a professor of anesthesiology and critical care at SSM Health Saint Louis University Hospital, Saint Louis, MO.
The authors report no conflict of interest.
REFERENCES
- Maraey A, Gupta K, Abdelmottaleb W, et al. National trends of structural heart disease interventions from 2016 to 2020 in the United States and the associated impact of COVID-19 pandemic. Curr Probl Cardiol. 2023;48:101526. PMID: 36455795.
- Bangalore S, Barsness GW, Dangas GD, et al. Evidence-based practices in the cardiac catheterization laboratory: a scientific statement from the American Heart Association. Circulation. 2021;144:e107–e119. PMID: 34187171.
- Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14:e275–e444. PMID: 28506916.
- O’Byrne ML, Millenson ME, Steven JM, et al. Operator-Directed procedural sedation in the congenital cardiac catheterization laboratory. JACC Cardiovasc Interv. 2019;12:835–843. PMID: 30981573.
- Kabra R, Girotra S, Vaughan Sarrazin M. Clinical outcomes of mortality, readmissions, and ischemic stroke among medicare patients undergoing left atrial appendage closure via implanted device. JAMA Netw Open. 2019;2:e1914268. PMID: 31664447.
- Reddy VY, Doshi SK, Kar S, et al. 5-year outcomes after left atrial appendage closure: from the PREVAIL and PROTECT AF trials. J Am Coll Cardiol. 2017;70:2964–2975. PMID: 29103847.
- FDA. Early Alert: WATCHMAN Access System issue from Boston Scientific. August 6, 2025. https://www.fda.gov/medical-devices/medical-device-recalls-and-early-alerts/early-alert-watchman-access-system-issue-boston-scientific. Accessed Nov 1, 2025.
- Kapadia SR, Yeh RW, Price MJ, et al. Outcomes with the WATCHMAN FLX in everyday clinical practice from the NCDR Left Atrial Appendage Occlusion Registry. Circ Cardiovasc Interv. 2024;17:e013750. PMID: 39056187.
- Ikoma T, Naruse Y, Kaneko Y, et al. Prevalence and characteristics of inspiration-induced negative left atrial pressure during pulmonary vein isolation. J Cardiovasc Dev Dis. 2023;10. PMID: 36975865.
- Saw J, Holmes DR, Cavalcante JL, et al. SCAI/HRS expert consensus statement on transcatheter left atrial appendage closure. Heart Rhythm. 2023;20:e1–e16. PMID: 36990925.
- Massalha E, Dakka A, Sabbag A, et al. Comparative analysis of anaesthesia modalities in pulmonary vein isolation: insights from a prospective multicentre registry. Europace. 2025;27. PMID: 39957475.
- Araujo B, Rivera A, de Oliveira Tapioca V, et al. Sedation vs. general anaesthesia in patients with atrial fibrillation undergoing catheter ablation: a systematic review and meta-analysis. Europace. 2025;27. PMID: 40966626.
- Miyazaki S, Kobori A, Sasaki Y, et al. Real-World safety profile of atrial fibrillation ablation using a second-generation cryoballoon in Japan: insight from a large multicenter observational study. JACC Clin Electrophysiol. 2021;7:604–613. PMID: 33640351.
- Gier C, Simon E, Ahmed A, et al. An ex vivo evaluation of air intrusion into pulsed field ablation sheaths during ablation and mapping catheter insertion. J Cardiovasc Electrophysiol. 2025;36:3231–3237. PMID: 41039826.
- Tsukahara K, Oginosawa Y, Fujino Y, et al. Prevention of serious air embolism during cryoballoon ablation; risk assessment of air intrusion into the sheath by catheter selection and change in intrathoracic pressure: an ex vivo study. J Cardiovasc Electrophysiol. 2019;30:2944–2949. PMID: 31588621.
- Miyazaki S, Hasegawa K, Mukai M, et al. Clinically manifesting air embolisms in cryoballoon ablation: can novel water buckets reduce the risk? JACC Clin Electrophysiol. 2020;6:1067–1072. PMID: 32972540.
- Takami M, Fujiwara R, Kijima Y, et al. Techniques for reducing air bubble intrusion into the left atrium during radiofrequency catheter and cryoballoon ablation procedures: An ex vivo study with a high-resolution camera. Heart Rhythm. 2019;16:128–139. PMID: 30075279.
