A 2025 quality improvement project at the University of Kentucky Medical Center redesigned the Neuro Interventional Radiology anesthesia workspace to address safety hazards like cramped spaces and cable clutter. The project aligns with evidence-based interventions and serves as a model for improving safety and efficiency in non-operating room anesthesia settings.
| Editor’s Note: The quality improvement project presented here reflects the experiences and practices of the authors’ institutions. While not prescriptive, they offer valuable insight and potential frameworks for improving patient safety. We encourage readers to use these examples as a starting point and adapt them within their own clinical settings. |
ADDRESSING SAFETY HAZARDS IN NORA ENVIRONMENTS
Non-Operating Room Anesthesia (NORA) environments, such as neurointerventional radiology (NlR) suites, are fraught with safety hazards that can compromise both patient care and anesthesiology professional well-being. Limited access to the patient, tangled cables, and cramped spaces create tripping risks, delay critical interventions like airway assessments, and heighten the potential for errors. As highlighted in the Anesthesia Patient Safety Foundation (APSF) Newsletter, an organized, hazard-free workspace that prioritizes unobstructed patient access is necessary to mitigate potential NORA patient safety threats.1 This call to action is echoed in the American Society of Anesthesiologists (ASA) statement on NORA services and the 2022 APSF Stoelting Conference, which urged anesthesia teams to lead transformative changes.2,3
At the University of Kentucky Medical Center, the Department of Anesthesiology, Perioperative, Critical Care, and Pain Medicine launched a quality improvement project to redesign the NIR anesthesiology workspace, drawing directly from evidence-based principles. Classified as a process improvement initiative (exempt from Institutional Review Board review), the effort aimed to expand space, streamline equipment, and eliminate clutter, ultimately fostering a safer, more efficient environment. This editorial shares the approach, key outcomes, and lessons for anesthesiology professionals navigating similar NORA constraints.
REDESIGNING THE NEUROINTERVENTIONAL RADIOLOGY ANESTHESIOLOGY WORKSPACE
This project began with a targeted survey of anesthesiology professionals within the Department of Anesthesiology (anesthesiologists, certified registered nurse anesthetists, and anesthesia residents) using the UK Department of Anesthesiology Provider Satisfaction with Unit Design Questionnaire (Figure 1). This tool captured quantitative ratings on a 1–5 Likert scale—focusing on safety and functionality across the induction, maintenance, and emergence phases of anesthesia alongside qualitative insights. The pre-intervention snapshot was stark: 88% of respondents reported barriers to optimal patient care, and 86% expressed dissatisfaction with their ability to provide care without harming themselves during procedures. “Optimal patient care” in this context refers to safe and timely access to the patient, especially the airway and vascular access sites, which were previously obstructed by equipment and cables. While 96% of anesthesia professionals surveyed endorsed the need for layout changes, the remaining 4% did not provide specific feedback, highlighting the need for more detailed follow-up in future surveys.
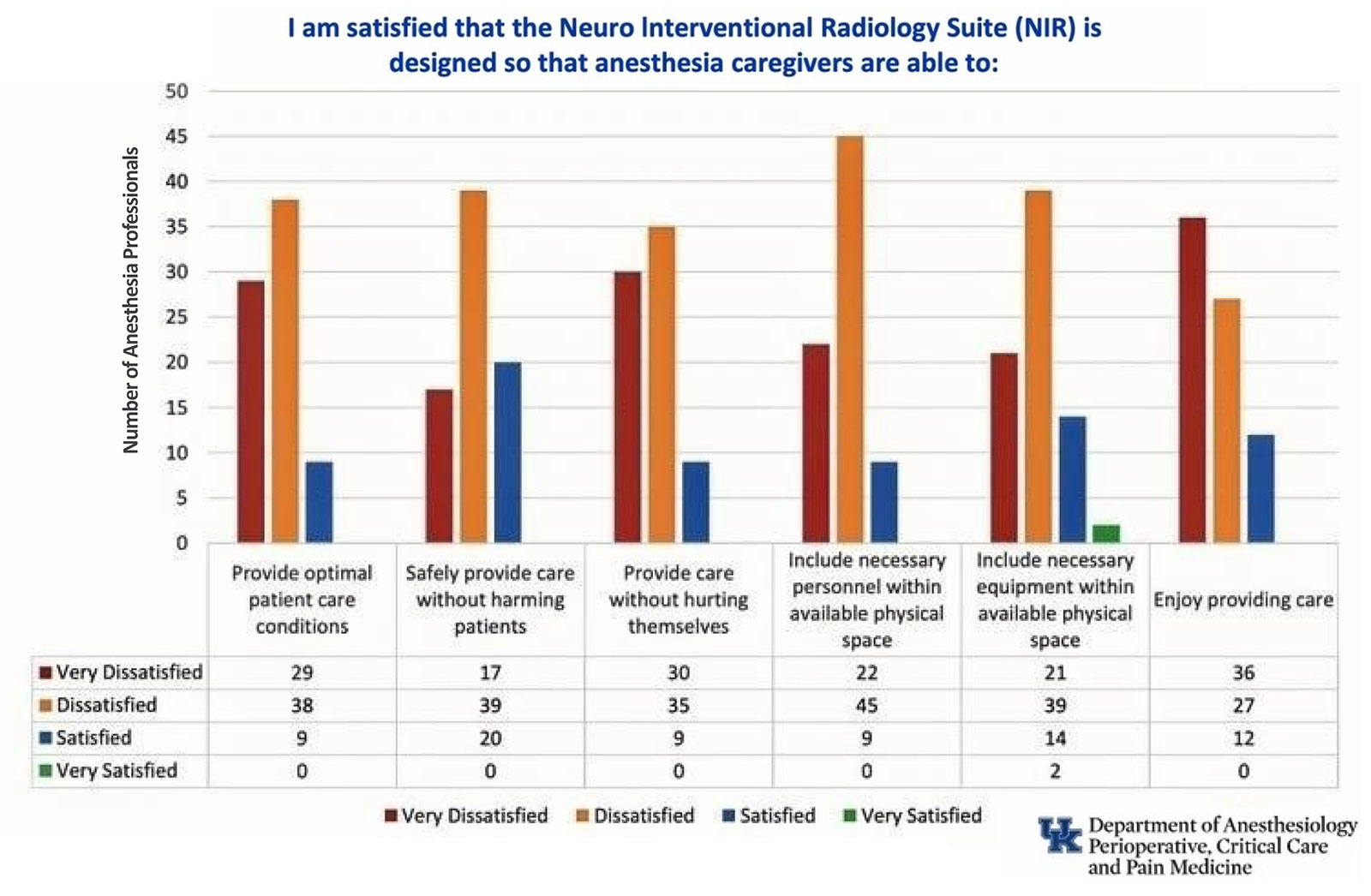
Figure 1: The University of Kentucky Department of Anesthesiology Provider Satisfaction with Unit Design Questionnaire. This was distributed prior to the intervention.
Qualitative feedback from survey respondents emphasized the severity of ergonomic and safety challenges:
- “Issues of frequently bumping into the monitor when providing care and having consistent availability of mobile lead shields. Having to crouch a lot to draw blood gases, check lines, etc…difficult ergonomics for body positions while doing procedures.”
- “One should not have to straddle a C-arm to reach the bag to ventilate a patient while simultaneously craning one’s neck to see the monitor.”
- “Navigating the equipment is unsafe to the cranium, the spine, and personal morale. There is no greater place for injuring anesthesia personnel.”
- “Very challenging to give superior care to patients with such a cramped and nonsensical layout.”
- “Many times, the IR monitor is in the direct walking path of the anesthesia professional. I must crawl to get to the arterial line transducer, patient, and other important items….inducing anesthesia alone is difficult.”
COLLABORATIVE REDESIGN FOR SAFER, MORE FUNCTIONAL SPACE
Guided by recommendations from the literature for adequate space (a minimum 85 square feet per ASA recommendations) and unimpeded access, we convened a multidisciplinary team of anesthesia staff, interventional radiologists, NORA personnel, and facility managers.2 Discussions prioritized low-disruption interventions: replacing an oversized anesthesia machine with a compact model, utilizing a pre-existing ceiling-mounted boom for cable management, and repositioning equipment to optimize the anesthesia environment. These changes expanded the workspace from a mere 14 square feet to 85 square feet—a six-fold gain that accommodated additional team members and equipment without crowding (Figures 2 and 3). To ensure buy-in, we incorporated hands-on staff training sessions, proactively addressing resistance by demonstrating real-time benefits, such as quicker arterial line insertions and reduced physical strain on anesthesia professionals.

Figure 2. Anesthesiology workspace prior to the intervention, at 14 square feet.
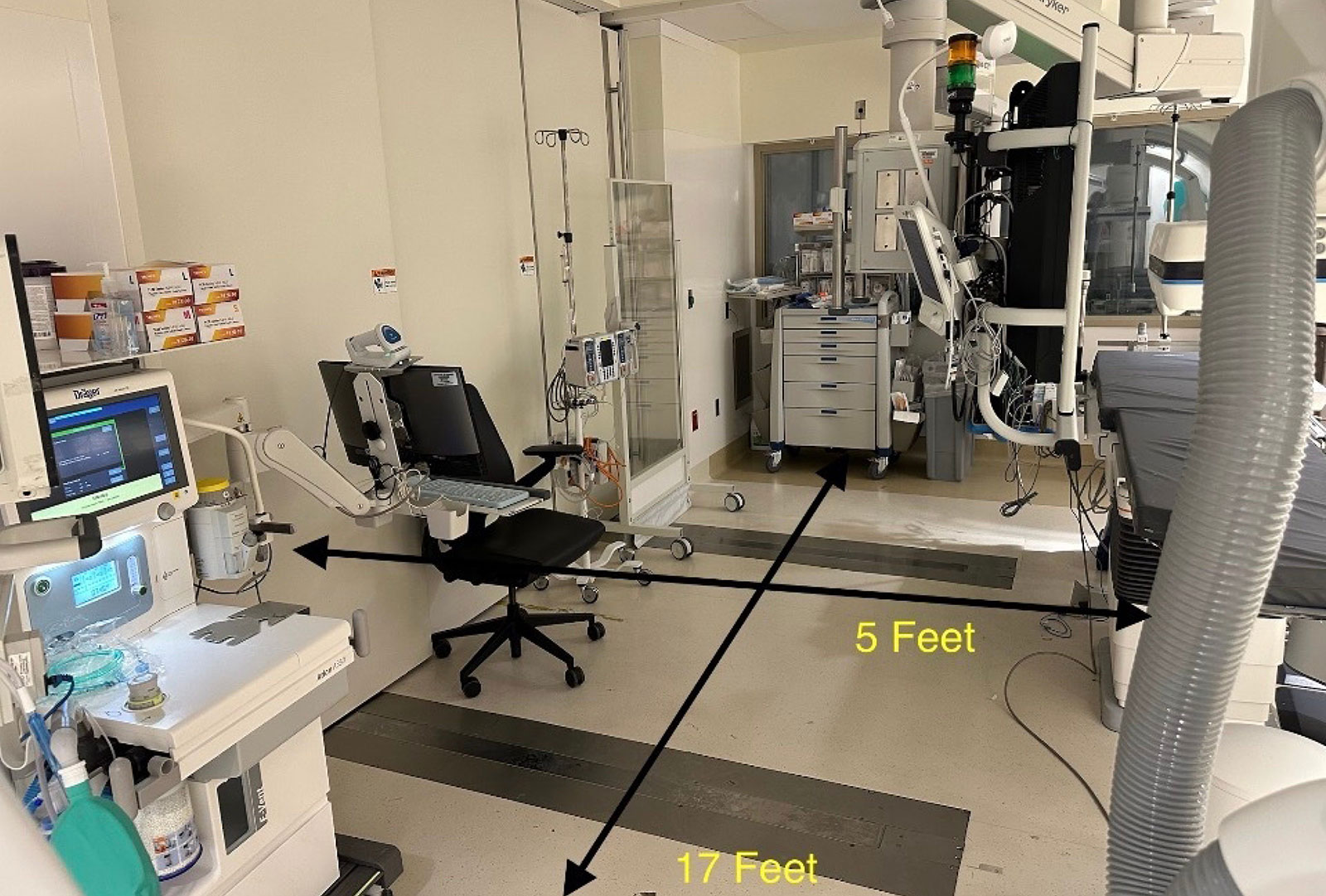
Figure 3. Anesthesiology workspace after the intervention, expanded to 85 square feet.
IMPROVED ACCESS, EFFICIENCY, AND PROVIDER SATISFACTION
The redesign yielded immediate, tangible improvements. Postimplementation feedback revealed noticeable changes: providers noted that the redesigned workspace dramatically improved their ability to move and operate within the suite. Previously, accessing the patient’s airway during the maintenance phase of anesthesia required navigating around equipment, taking up to 22 steps. After the redesign, that distance was reduced to a single step, allowing one anesthesia professional to assess and manage the airway independently, eliminating the need for a second provider and enabling faster, safer responses to airway concerns. Additional feedback praised the new layout for offering a larger, less cluttered space to deliver patient care. These gains not only streamlined induction, maintenance, and emergence, but also boosted overall satisfaction, aligning with the APSF’s vision of anesthesia care that safeguards both patients and clinicians.4
LESSONS LEARNED: KEY STRATEGIES FOR SUCCESSFUL REDESIGN
The success of the redesign was driven by early engagement with frontline anesthesia clinicians, whose firsthand insights helped identify specific hazards and practical solutions. By leveraging existing infrastructure such as the ceiling-mounted boom and compact anesthesia machine, the team minimized costs and avoided interruptions to clinical operations. Importantly, the redesign was implemented without disrupting the scheduling of cases in the NIR suite, ensuring continuity of patient care. Collaboration with departmental leadership and facility managers helped align the project with institutional goals and facilitated smooth execution. Moving forward, incorporating formal tracking of safety incidents and establishing regular feedback mechanisms will be essential to sustaining improvements and guiding future redesigns.
CONCLUSION: A MODEL FOR SAFER ANESTHESIA CARE IN NORA SETTINGS
Our quality improvement project successfully transformed the NIR suite into a more efficient workspace and enhanced safety for patients and anesthesia providers. By addressing key risks such as cramped spaces, cable clutter, and restricted access through evidence-based redesign elements, we created a safer and more functional environment. The project’s alignment with recent publications from the ASA and APSF positions it as a model for health care institutions expanding NORA services. This initiative underscores the vital role of intentional workspace optimization in advancing patient and provider safety, offering a blueprint for transformative change in anesthesia care delivery.
John M. Edwards, CRNA, DNAP, is a staff CRNA at the University of Kentucky Department of Anesthesiology, Lexington, KY.
Stace D. Dollar, CRNA, DNAP, is a staff CRNA at the University of Kentucky Department of Anesthesiology, Lexington, KY.
Syed Z. Ali, MD, FASA, is an associate professor of anesthesiology, University of Kentucky Department of Anesthesiology, Lexington, KY.
The authors report no conflicts of interest.
REFERENCES
- Chang C, Tan J, Fogarty Mack P, Anca D. Clinician safety in NORA. APSF Newsletter. 2023; 38:84–86. https://www.apsf.org/article/clinician-safety-in-nora/ Accessed March 13, 2026.
- American Society of Anesthesiologists. Statement on nonoperating room anesthesia services. https://www.asahq.org/standards-and-practice-parameters/statement-on-nonoperating-room-anesthesia-services Accessed August 16, 2025.
- Beard J, Methangkool E, Angus S, et al. Consensus recommendations for the safe conduct of nonoperating room anesthesia: a meeting report from the 2022 Stoelting Conference of the Anesthesia Patient Safety Foundation. Anesth Analg. 2023;137:e8–e11. PMID: 37224074.
- Anesthesia Patient Safety Foundation. APSF mission, vision and values. APSF. https://www.apsf.org/about-apsf/mission-vision-values/ Accessed October 4, 2025.
