Episode #275 Tracheostomy and Laryngectomy Patient Safety: Bedside Signs, Algorithms, and the Discipline that Prevents Catastrophe
October 8, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
This is Part 2 of 2 in our series. Our featured article again today is “Keeping Patients Safe During Emergency Tracheostomy Management” by Jack Buckley, MD.
Here is the citation for the article that we talked about on the show today:
- Brenner MJ, Cramer JD, McGrath BA, et al. Oral intubation attempts in patients with a laryngectomy: a significant safety threat. Otolaryngol Head Neck Surg. 2021; 164:1040–1043. PMID: 33048019.
Check out Figure 5 in the article:
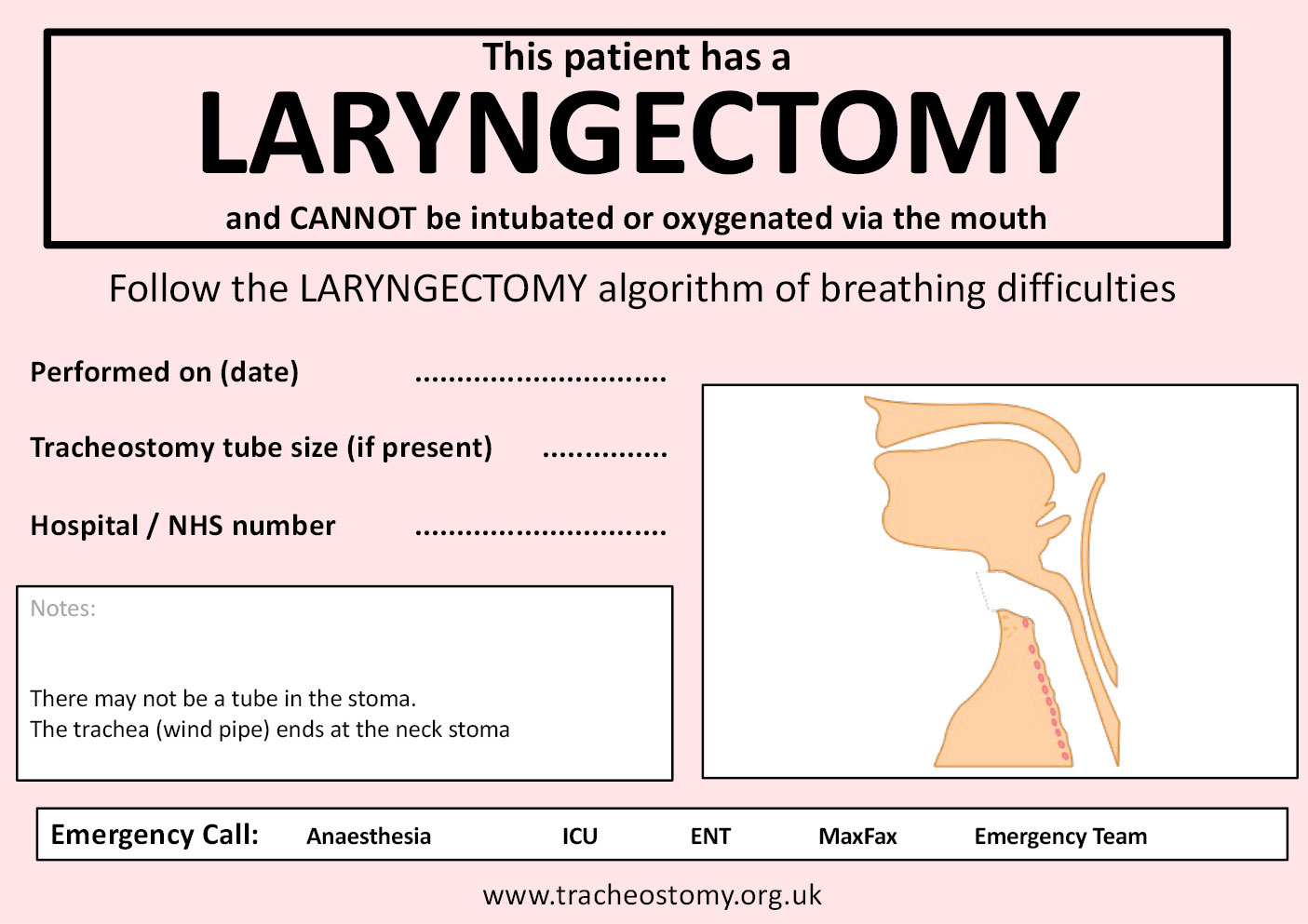
Figure 5: Laryngectomy bedside sign. Used with permission from Brendan McGrath and the National Tracheostomy Safety Project.
Check out Figure 6 in the article for an emergency algorithm to help manage patients who have had a laryngectomy.
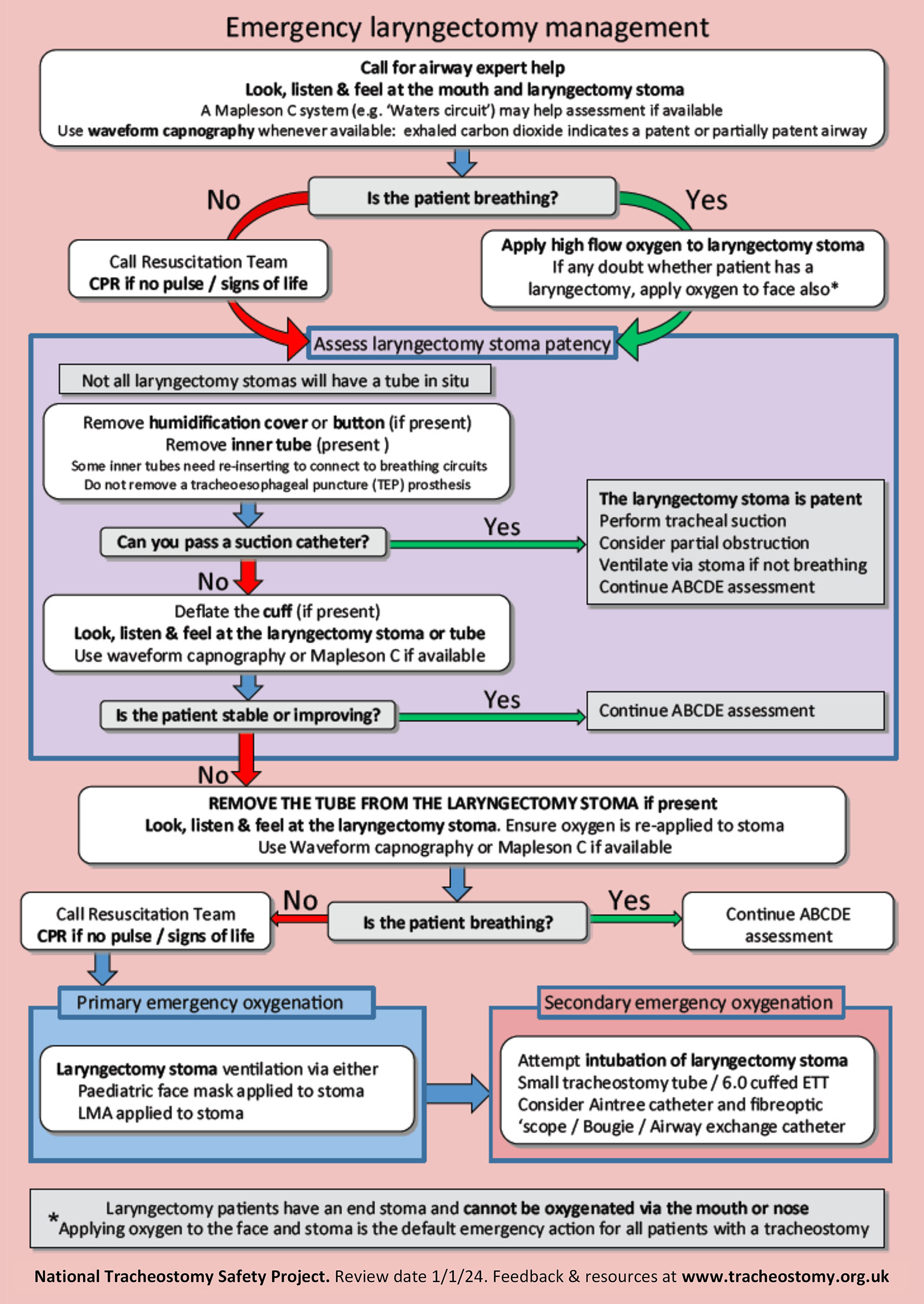
Figure 6: Laryngectomy management algorithm. Used with permission from Brendan McGrath and the National Tracheostomy Safety Project.
You can watch the recorded sessions from the 2025 APSF Stoelting Conference on Transforming Maternal Care.
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We hope you tuned in last week for the first part of our two-part series on keeping patients safe during emergency tracheostomy management. Last week, we talked about an emergency algorithm for a malfunctioning tracheostomy and the importance of bedside signs for patients with tracheostomies. This week we are covering what to do when a patient presents to the operating room with a tracheostomy in place for a different surgical procedure and special considerations for patients with laryngectomies.
Before we dive further into the episode today, we’d like to recognize Solventum, a major corporate supporter of APSF. Solventum has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Solventum – we wouldn’t be able to do all that we do without you!”
Our featured article again today is “Keeping Patients Safe During Emergency Tracheostomy Management”
by Jack Buckley. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue and then scroll down until you get to our featured article today. You can also find the June 2025 APSF Newsletter in the Newsletter archives. Don’t worry, I will include a link in the show notes as well.
Have you provided anesthesia care for a patient undergoing tracheostomy? Have you had to troubleshoot a malfunctioning tracheostomy before? Does your hospital use bedside signs for all patients with tracheostomies in place? There are so many resources available in this article to help keep your patients safe.
Let’s do a quick review of the Tracheostomy bedside sign. This is Figure 4 in the article. The bedside sign should accompany patients with tracheostomies throughout their hospital stay.
The sign says that “This patient has a tracheostomy.” There is a potentially patent upper airway (intubation may be difficult). Then, you can circle surgical or percutaneous for the type of tracheostomy with the following information:
- Performed on (date)
- Tracheostomy tube size (if present)
- Hospital NHS number
- There is a picture of the different types of tracheostomies including percutaneous, Bjork flap, and slit type
- There are notes on the card to help fill out the card that state: Indicate tracheostomy type by circling the relevant figure. Indicate location and function of any sutures. Laryngoscopy grade and notes on upper airway management. Any problems with this tracheostomy. Then in case of emergency call Anesthesia, ICU, ENT, Maxfax, and Emergency Team.
For more information, you can head over to tracheostomy.org.uk and check out the show notes for more details.
Now, it’s time to get back into the article where we left off. When was the last time you provided anesthesia care for a patient presenting to the operating room with a tracheostomy in place? What was your plan for airway management? There are several considerations. First, we need to obtain a tracheostomy history. Does the patient have a patent upper airway? When was the tracheostomy placed, etc.?
Next, we need to know what the ventilation needs are for the procedure. The simplest option is to use a cuffed tracheostomy that will not be in the surgical field. You can use this without needing to make any changes. If there is an uncuffed tracheostomy, this may be used if positive pressure ventilation is not indicated and the procedure can be completed with spontaneous ventilation. This is a decision point: Is positive pressure ventilation going to be required during the procedure? It is also important to determine if the tracheostomy tube will be in the surgical field. Then, you may need to replace the tracheostomy tube with an endotracheal tube that is placed through the mouth or the tracheostomy stoma. Here is another decision point: Do you need to replace the tracheostomy tube with an endotracheal tube and how will you accomplish this? Important considerations for attempting oral intubation include:
Inexperience with replacing tracheostomies
History of easy intubation
No oropharyngeal pathology present
New tracheostomy. Remember, a new surgical tracheostomy is less than 4 days old and less than 7-10 days for percutaneous tracheostomy.
Factors in support of intubating through the tracheostomy stoma include the following:
- Comfort with replacing a tracheostomy
- History of difficult intubation
- Known oropharyngeal pathology that will make oral intubation difficult
- A mature tracheostomy with a well-healed stoma
Following oral intubation, the cuff of the endotracheal tube should be placed just beyond the stoma site to create a seal with the trachea. A wire-reinforced endotracheal tube may need to be used for intubation through the stoma site to decrease the risk for kinking. The tracheal stoma is usually positioned between the 2nd-4th tracheal ring and the distance from the stoma to the carina is about 6.5 cm, so you need to be careful to avoid placing the endotracheal tube in the mainstem bronchus. It is important to listen for bilateral breath sounds after endotracheal tube placement to ensure proper position and make any changes if needed before the procedure starts. Remember, if there are any concerns for difficult placement of the endotracheal tube through the stoma, then you may want to use an airway exchange catheter to facilitate the exchange of the tracheostomy tube. This is a good option for patients with a fresh tracheostomy. Using the exchange catheter helps to minimize the risk of creating a false passage in the subcutaneous tissue with the endotracheal tube. Some exchange catheters also have an open channel to allow for insufflation of oxygen during the exchange to help decrease the risk for desaturation.
Now we have a laryngectomy patient presenting to the operating room. There are special considerations for providing safe anesthesia care for these patients who have had their larynx surgically removed and their trachea sutured to the skin of the anterior neck. As a result, the trachea does not communicate with the oropharynx, which means that patients cannot be orally intubated, or mask ventilated through the oropharynx. Anesthesia professionals need to remain vigilant especially in the setting of respiratory distress. Let’s look at the literature on this. There is a 2021 article by Brenner and colleagues, “Oral intubation attempts in patients with a laryngectomy: a significant safety threat.” The results revealed that over half of the US otolaryngologists who responded to this study reported cases of attempted oral intubations in patients with laryngectomy with a resultant mortality rate of 26%. Similar results were found in the UK as well with failed resuscitation leading to increased morbidity and mortality. The authors of this study highlight the need for staff education, patient engagement, effective signage, systems-based practices, and necessary resources as critical steps for safe airway management for laryngectomy patients.
The first step for improving patient safety is to highlight that laryngectomy patients do not have a patent upper airway. This can be done with a bedside sign for all laryngectomy patients as well as placing an alert in the electronic medical record. Let’s check out Figure 5 in the article for an example of a bedside sign. The sign states: This patient has a :Laryngectomy and CANNOT be intubated or oxygenated via the mouth. Below that it states: Follow the Laryngectomy algorithm of breathing difficulties. Then, you can put information about the date of the procedure, tracheostomy tube size if present and the hospital number. There is also an anatomical picture which shows the disconnection and space for notes with two important points highlighted: There may not be a tube in the stoma. The trachea ( windpipe) ends at the neck stoma. At the bottom of the card is information about who to call for an emergency. For more information about this bedside card, head over to www.tracheostomy.org.uk and check out the show notes for more details.
Now it’s time to talk about management strategies for total laryngectomy patients who experience respiratory distress. The first step is to apply an oxygen mask over the stoma site. A paediatric mask may be placed over the stoma site to provide mask ventilation. Keep in mind that most patients with a total laryngectomy do not have a cuffed tracheostomy tube in place. A cuffed tracheostomy tube or appropriately sized endotracheal tube can be placed in the stoma in the neck to provide positive pressure ventilation if needed. The tube should advance easily into the trachea since most patients have a reasonably sized stoma. Since the trachea is sutured to the skin during the laryngectomy, it is more difficult to advance the tube into a false passage even after the sutures have been removed. Once again, having an algorithm for the management of respiratory distress for laryngectomy patients can be helpful to provide safe care especially during a time-critical emergency event.
Check out Figure 6 in the article for an example. We are going to review it now! The first step is to call for airway expert help and then look, listen, and feel at the mouth and laryngectomy stoma. Use waveform capnography whenever available since exhaled carbon dioxide indicates a patent or partially patent airway. The first question is, Is the patient breathing? If Yes, then apply high flow oxygen to laryngectomy stoma and if there is any doubt about whether the patient has a laryngectomy, also apply oxygen to the face. If No, call the resuscitation team and begin CPR if needed. The next step is to assess the laryngectomy stoma for patency. Not all laryngectomy stomas will have a tube present.
First, remove the humidification cover or button if present and remove the inner liner if present.
Some inner liners will need to be re-inserted to connect with the breathing circuit.
Do NOT remove the tracheoesophageal puncture prothesis if present.
Now, can you pass a suction catheter? If Yes, the laryngectomy stoma is patent. Perform suction, consider partial obstruction, ventilate via the stoma if not breathing, and continue to assess the patient. If No, deflate the cuff if present and look, listen, and feel at the stoma. Is the patient stable or improving? If Yes, continue your assessment. If No, remove the tube from the laryngectomy stoma if present and look, listen, feel, at the stoma site while using waveform capnography if available.
Is the patient breathing now? If Yes, continue your assessment. If No, call the resuscitation team begin CPR if needed. The steps for primary emergency oxygenation include ventilation with a paediatric face mask or LMA applied to the stoma. Secondary emergency oxygenation involves attempted intubation thru the laryngectomy stoma with a 6.0 cuffed endotracheal tube or a small tracheostomy tube. Consider using the Aintree catheter, bougie, or fibreoptic scope if needed. At the bottom of the resuscitation algorithm is the statement: Laryngectomy patients have an end stoma and cannot be oxygenated via the mouth and nose. Applying oxygen to the face and stoma is the default emergency action for all patients with a tracheostomy. You can check out this algorithm in the article and in the show notes for more details. This is an excellent resource to have available anytime you are providing care for a patient with a total laryngectomy.
We made it to the end of the article. Buckley reminds us that patients with tracheostomy are commonly seen in clinical practice and we need to be prepared since complications can occur. By understanding the management steps that we talked about over the past two shows, anaesthesia professionals can help to keep patients safe from harm related to their artificial airway. Bedside signs and emergency management algorithms are excellent tools to provide the necessary information for safe care in the setting of respiratory distress and a malfunctioning surgical airway.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
Our podcast series on the 2025 APSF Stoelting Conference is coming up. If you just can’t wait to learn more about transforming maternal care, we hope that you will check out the recordings from the conference which are up now. Head over to APSF.org and click on the Conferences and Events heading. Then select APSF Stoelting Conference 2025 where you see the recordings. You can also check out the recordings on the APSF YouTube Channel. There is so much to learn about improving maternal patient safety and we hope that you will check it out.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
