Episode #274 Critical Decision Points in Emergency Tracheostomy Management
October 1, 2025
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is from the June 2025 APSF Newsletter. It is “Keeping Patients Safe During Emergency Tracheostomy Management” by Jack Buckley, MD.
Here is the citation for the article that we reviewed on the show today.
Spataro E, Durakovic N, Kallogjeri D, Nussenbaum B. Complications and 30-day hospital readmission rates of patients undergoing tracheostomy: a prospective analysis. Laryngoscope. 2017;127:2746–2753. PMID: 28543108.
Check out Figures 3 and 4 from the article. These are excellent tools to help keep patients with tracheostomy safe.
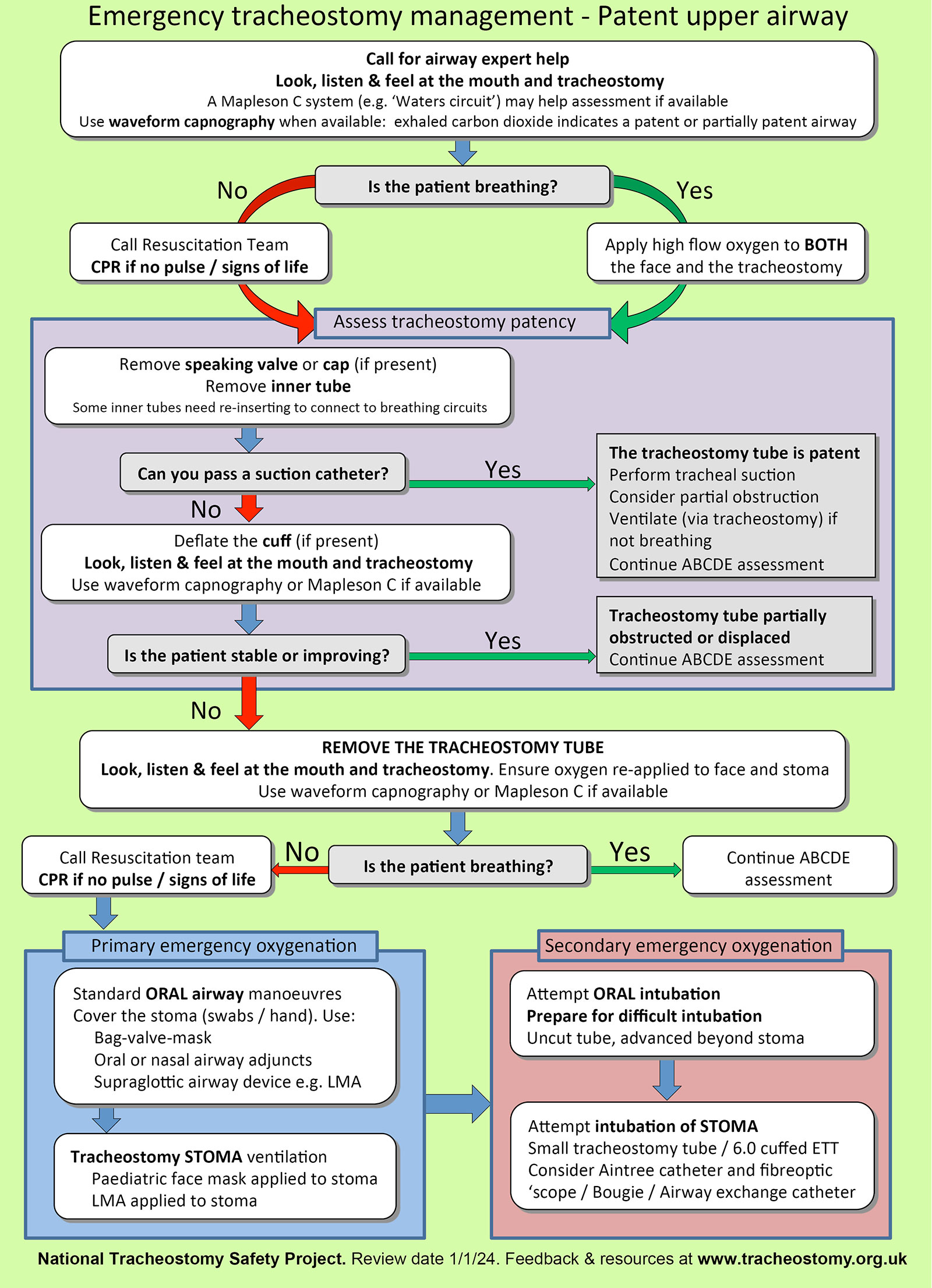
Figure 3: Emergency tracheostomy management algorithm. Used with permission from Brendan McGrath and the National Tracheostomy Safety Project.
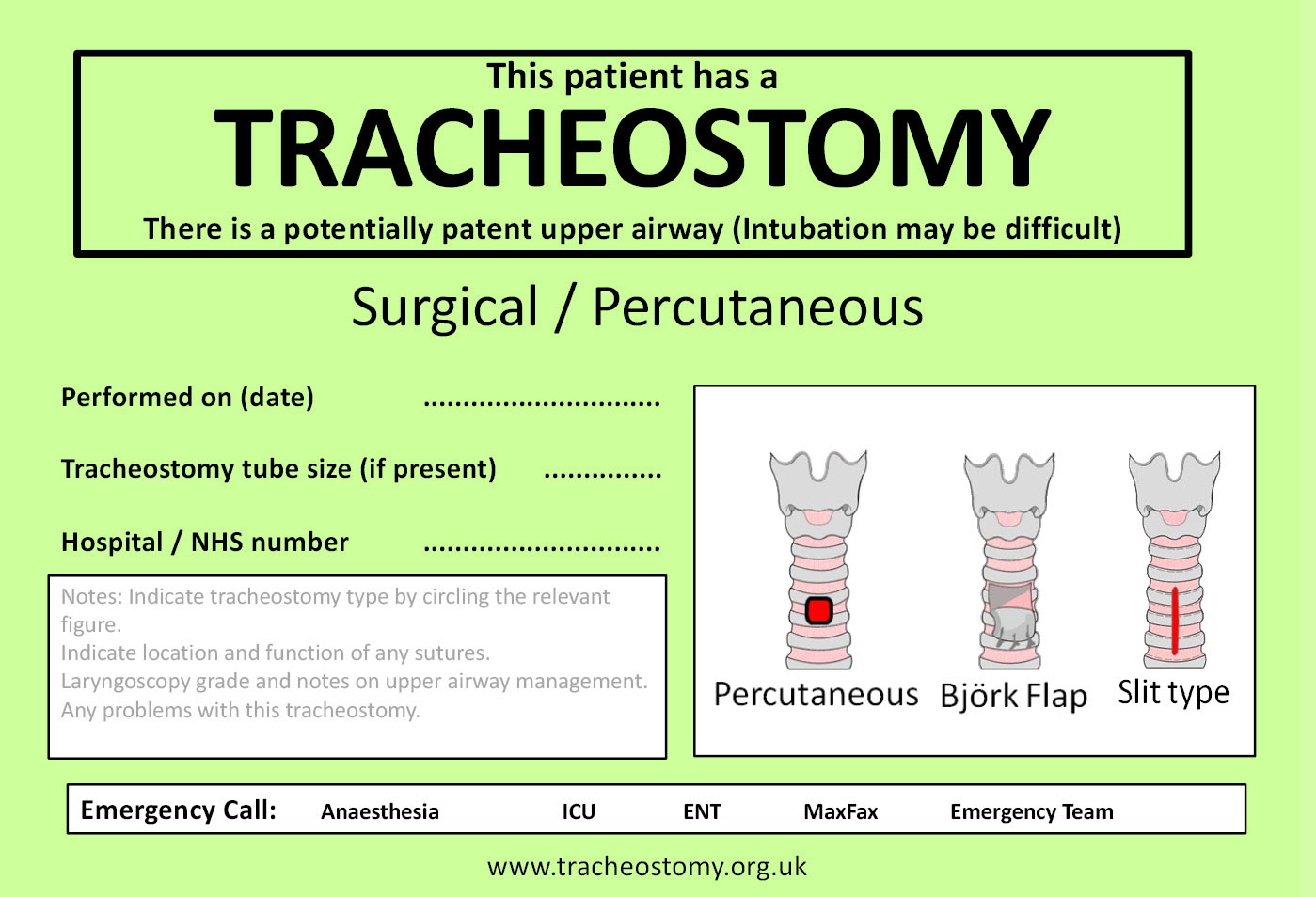
Figure 4: Tracheostomy bedside sign. Used with permission from Brendan McGrath and the National Tracheostomy Safety Project.
Check out www.tracheostomy.org.uk for more information.
This episode was edited and produced by Mike Chan.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2025, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. For our show today, we are continuing to cover the excellent articles from the June 2025 APSF Newsletter, but first up we have a sneak peek from the 2025 APSF Stoelting Conference on Transforming Maternal Care: Innovations and Collaborations to Reduce Morbidity and Mortality.
[Stoelting Conference Clip]
If you want to hear more, you can check out the livestream by heading over to APSF.org and clicking on the Conferences and Events heading. Then select APSF Stoelting Conference 2025 where you see the recordings. You can also check out the APSF YouTube Channel and keep downloading this podcast because we will have an upcoming Stoelting Conference Podcast series that you don’t want to miss.
Before we dive further into the episode today, we’d like to recognize GE Healthcare, a major corporate supporter of APSF. GE Healthcare has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, GE Healthcare – we wouldn’t be able to do all that we do without you!”
Our featured article today is “Keeping Patients Safe During Emergency Tracheostomy Management”
by Jack Buckley. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue and then scroll down until you get to our featured article today. You can also find the June 2025 APSF Newsletter in the Newsletter archives. Don’t worry I will include a link in the show notes as well.
Have you provided anesthesia care for a patient undergoing tracheostomy? Patients may need a tracheostomy for prolonged mechanical ventilation, inability to protect their airway, or upper airway obstruction from pathology of the oropharynx. Complications following this procedure are common so you may have also been called on to provide anesthesia care for a patient with a malfunctioning tracheostomy. There is a 2017 single center study of 100 patients undergoing tracheostomy that revealed a complication rate of almost 50% during the initial hospitalization. Here is the breakdown of complications: tracheostomy obstruction 19%, bleeding 16%, infection 14%, and accidental decannulation 13%. Anesthesia professionals need to be prepared for these complications to help keep patients with tracheostomies safe. We are going to go through the management steps of a potentially malfunctioning tracheostomy as well as what to do when a patient presents to the operating room with a tracheostomy in place for a different surgical procedure, and special considerations for patients with laryngectomies. Here we go!
Patients undergoing mechanical ventilation may have occlusion or accidental decannulation of their tracheostomies leading to high airway pressures or loss of tidal volume and loss of end-tidal carbon dioxide. This is a serious concern and it is important to troubleshoot quickly to determine the cause and intervene prior to patient deterioration. The first step is to deflate the tracheostomy cuff to allow for spontaneous breathing if possible. At the same time, you need more information about the tracheostomy:
How long ago was it placed?
What was the indication?
What is the type of tracheostomy, surgical or percutaneous.
Next up, determine if the patient has a patent upper airway for mask ventilation or oral intubation and consider the potential for a difficult oral intubation as well.
For spontaneously breathing patients who are moving air well around the deflated cuff, you can place an oxygen mask on the patient’s mouth or tracheostomy stoma to provide supplemental oxygen and monitor ventilation with waveform capnography.
The next step is to make sure there is no obstruction. You can remove the inner cannula, if it is there. The inner cannula should be easy to remove for cleaning of mucous and other materials which may occlude the tracheostomy tube. Check out Figure 1 in the article for a picture of a cuffed tracheostomy, an obturator that is used to help with placement of the tracheostomy, and the removable inner cannula.
If ventilation is still not adequate, it is time to suction through the tracheostomy tube with a suction catheter into the distal trachea. This is also a good test for an occlusion or malposition. If the suction catheter does not advance beyond the end of the tracheostomy, then the tip of the tracheostomy may be positioned against the tracheal wall or be occluded by an overinflated cuff.
Ventilation is still not adequate, so we need to continue to troubleshoot. If the suction catheter does not advance beyond the tip of the tracheostomy, the tracheostomy may have become displaced from the trachea and now be positioned in the subcutaneous tissue in the neck. We need to know where the tracheostomy tube is now located. At this point, you may want to attempt to gently provide positive pressure ventilation with a bag-valve-mask. If end-tidal CO2 is not present or there are high airway pressures, then the tracheostomy tube is most likely no longer in the trachea. Time to grab a bronchoscope, if available, and advance down the tracheostomy tube to confirm the location. Keep in mind that continued attempts at positive pressure ventilation with a tracheostomy tube that has migrated to the subcutaneous space may cause serious complications including subcutaneous emphysema, pneumothoraces, pneumomediastinum, and difficult intubation since the pressurized air can track into the subcutaneous tissues of the upper airway. Check out Figure 2 in the article for a Chest Xray of a patient with a mal-positioned tracheostomy tube who received positive pressure ventilation leading to a pneumothorax on the left and subcutaneous emphysema in the neck.
So, now we have a tracheostomy tube that may be in the subcutaneous tissue and our patient is not ventilating adequately. It is time to remove the tracheostomy. The next step is to evaluate ventilation again through the stoma and orally. If ventilation is adequate, then we are on a non-emergent pathway and can wait for additional help to arrive.
If ventilation is inadequate and the patient is desaturating, the next step is to attempt mask ventilation orally while occluding the stoma or through the tracheostomy stoma. You may consider using a pediatric mask for a better fit while attempting ventilation through the stoma.
If mask ventilation remains inadequate, it is time to move on to oral intubation or via the tracheostomy stoma. Keep in mind that the decision of where to intubate depends on the following:
Patent upper airway
Expected difficulty of oral intubation
Experience of clinicians present
Age of the tracheostomy
Here are some of the factors that support oral intubation:
Inexperience in replacing tracheostomies
History of easy oral intubation
No oropharyngeal pathology present
If it is a new tracheostomy which includes a surgical tracheostomy less than 4 days or percutaneous tracheostomy less than 7-10 days. With a fresh tracheostomy stoma there is a risk of inadvertently advancing the tube into the subcutaneous tissue and creating a false track.
A surgical tracheostomy matures earlier because the surgical tracheostomy has a portion of the trachea that is sutured to the skin which decreases the risk of advancing a tube into the subcutaneous tissue.
Here are some of the factors that support intubation through the tracheostomy stoma instead of oral intubation:
Comfort and experience with replacing a tracheostomy
History of difficult intubation or known oropharyngeal pathology that will make oral intubation difficult
A mature tracheostomy with a well-healed stoma.
If the stoma is mature with a moderate sized opening and a clear path to the trachea, then the tracheostomy tube can be simply advanced back into the trachea.
If the stoma is small or difficultly is expected, then an endotracheal tube is recommended since it may be less likely to advance into a false passage.
An intubation bougie can be placed into the stoma first and used to feel for tracheal rings in a fashion similar to oral intubation.
Another option is to use a bronchoscopy scope to advance into the stoma first while attempting to identify the trachea.
We just covered an emergency algorithm for the management of a patient with a malpositioned tracheostomy tube and failed ventilation. Anesthesia professionals need to remain vigilant. Bedside signs and algorithm sheets that are readily available to help management these patients can be lifesaving.
Check out Figure 3 and 4 in the article. Figure 3 is an algorithm for emergency tracheostomy management for a patient with a patent upper airway. Figure 4 is a tracheostomy bedside sign. These are excellent tools. You can have these available anytime you are providing anesthesia care for a patient with a tracheostomy and may be useful in other hospital departments including the ICU and Emergency department. The bedside sign should accompany patients with tracheostomies throughout their hospital stay.
The sign says that “This patient has a tracheostomy.” There is a potentially patent upper airway (intubation may be difficult). Then, you can circle surgical or percutaneous for the type of tracheostomy with the following information:
Performed on (date)
Tracheostomy tube size (if present)
Hospital NHS number
There is a picture of the different types of tracheostomy including percutaneous, Bjork flap, and slit type
There are notes on the card to help fill out the card that state: Indicate tracheostomy type by circling the relevant figure. Indicate location and function of any sutures. Laryngoscopy grade and notes on upper airway management. Any problems with this tracheostomy. Then in case of emergency call Anesthesia, ICU, ENT, Maxfax, and Emergency Team.
For more information, you can head over to tracheostomy.org.uk and I will include these figures in the show notes and the link as well.
Figure 3 covers emergency tracheostomy management. Let’s go through it now.
The first step is to call for airway expert help. Then, look, listen, feel at the mouth and tracheostomy. A Mapleson C system may help assess if available and waveform capnography should be used. Exhaled carbon dioxide indicates a patient or partially patent airway.
The next question is: Is the patient breathing? If Yes, you are on the green pathway and you can apply high flow oxygen to BOTH the face and tracheostomy. IF no, you are on the red pathway and you need to call the resuscitation team and begin CPR if there is no pulse.
Both pathways converge on assessment of tracheostomy patency which involves removing the speaking valve or cap, removing the inner tube, but remember that some inner tubes will need to be reinserted to connect to the breathing circuit.
The next question is: Can you pass a suction catheter? If Yes, then the tracheostomy tube is patent. Follow-up steps include suction the trachea, consider partial obstruction, ventilate via the tracheostomy if not breathing, and continue to assess the patient. If no, then deflate the cuff and evaluate at the mouth and tracheostomy site again or use waveform capnography if available.
The next question is: Is the patient stable or improving? If Yes, then the tracheal tube is partially obstructed or displaced and you can continue to assess the patient. If No, remove the tracheostomy tube and evaluate at the stoma site and mouth again while making sure to provide supplemental oxygen. Is the patient breathing now? If Yes, then continue your assessment. If No, call for the resuscitation team and begin CPR if needed.
For primary emergency oxygenation, use standard oral airway maneuvers. Cover the stoma with swabs or a hand and use bag-valve-mask, oral or nasal airway adjuncts, or a supraglottic airway device. You may consider tracheostomy stoma ventilation with a pediatric face mask or an lma applied to the stoma.
For secondary emergency oxygenation, attempt oral intubation, prepare for difficult intubation, advance tube beyond the stoma. Attempt intubation a the stoma with a small tracheostomy tube or a 6.0 cuffed endotracheal tube, consider using an Aintree catheter, fiberoptic bronchoscope, bougie, or airway exchange catheter to help place endotracheal tube. This algorithm is from the National Tracheostomy Safety Project and I will include it in the show notes as well.
There is still more to talk about when it comes to emergency tracheostomy management, but you will need to tune in next week. Make sure you like, subscribe, and download the Anesthesia Patient Safety podcast so you don’t miss it.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
The APSF Newsletter is the official journal of the Anesthesia Patient Safety Foundation. Readers include anesthesia professionals, perioperative providers, key industry representatives, and risk managers. It is free of charge and available in a digital format with a focus on anesthesia-related perioperative patient safety issues. The 40th Anniversary of the APSF Newsletter is right around the corner and we will have a special newsletter publication!! That’s right. All new articles, the latest in perioperative patient safety, and more ways for you to help to keep yourself and your patients safe!
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2025, The Anesthesia Patient Safety Foundation
