Episode #233 Revolutionizing Anesthesia: The Impact of Remimazolam
December 18, 2024
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
We are returning to the October 2023 APSF Newsletter today and revisiting our earlier episodes (#175 and #176) on Remimazolam. Our featured article is “Remimazolam: Patient Safety Considerations of a Novel, Practice-Changing Drug in Perioperative Medicine” by Arnoley Abcejo and Miguel Teixeira.
Practical Clinical Considerations:
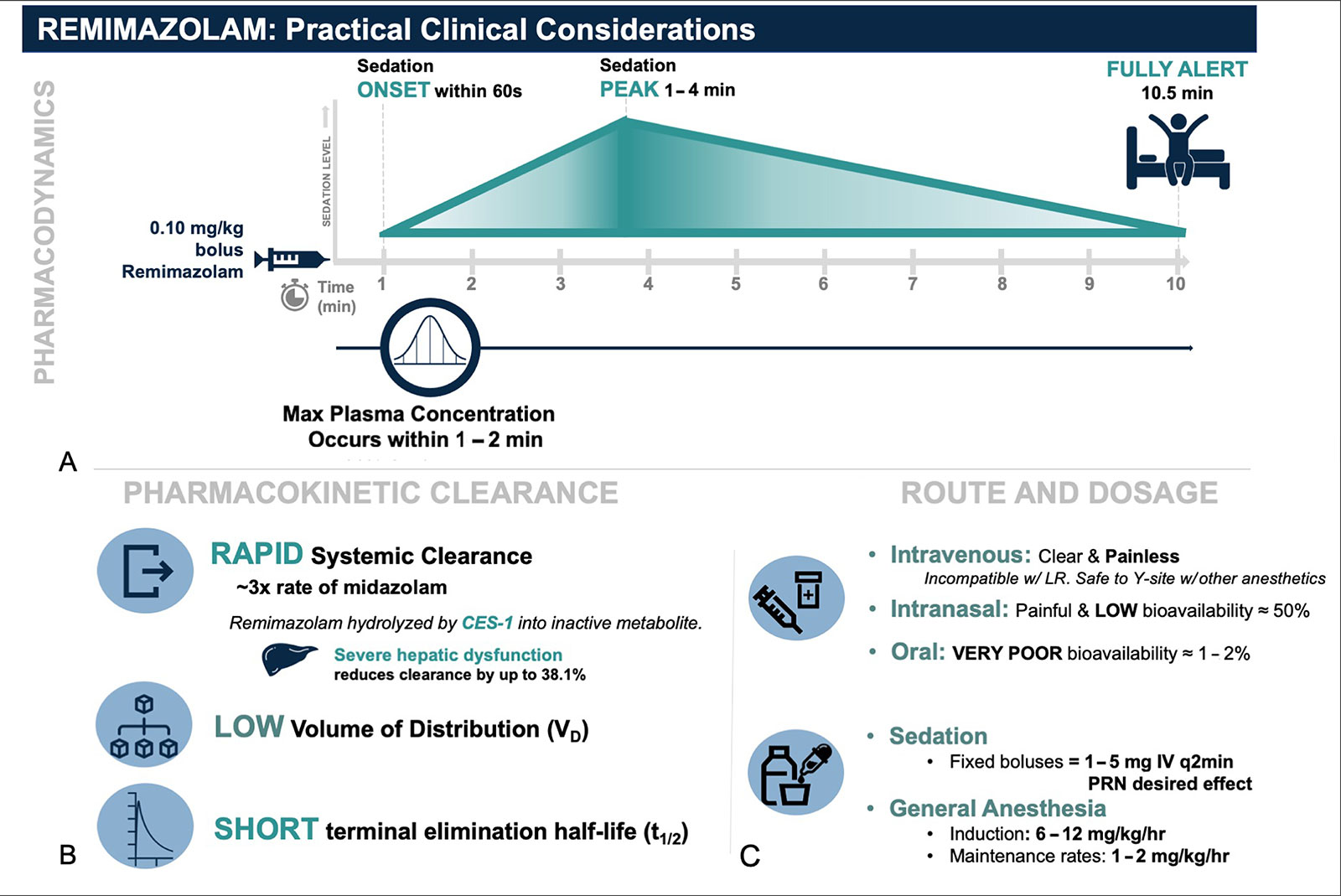
Figure 2: Remimazolam pharmacokinetic and pharmacokinetic profile adapted with permission from Figure 2 from Teixeira et al. “The role of remimazolam in neurosurgery and in patients with neurological diseases: a narrative review.” J Neurosurg Anesthesiol, May 31, 2023.
Abbreviations: mg = milligram, kg = kilogram, hr = hour.
Common adverse reactions following remimazolam administration:
- Heart rate and blood pressure changes
- Body movement
- Nausea
- Dizziness
- Headaches
Contraindications to Remimazolam Administration:
Known severe hypersensitivity reaction to Dextran 40
Clinical Practice Considerations:
- For patients with complex cardiovascular or hemodynamically unstable patients:
- Limited impact on respiratory depression, systemic vascular tone, and inotropic, dromotropic, and chronotropic function.
- For non-operating room anesthesia or NORA procedures:
- GI and Pulmonary Endoscopic Procedures
- Interventional Radiology Procedures
- Magnetic Resonance Imaging
- For neurosurgical procedures:
- Rapid amnestic sedation and anxiolysis followed by neurologic exam
- Awake craniotomies during pin placement, local anesthetic administration, urethral catheter placement, and surgical incision
Here are a few citations to recently published articles on Remimazolam. We hope that you will check them out.
- Fechner, J.; El-Boghdadly, K.; Spahn, D.R.; Motsch, J.; Struys, M.; Duranteau, O.; Ganter, M.T.; Richter, T.; Hollmann, M.W.; Rossaint, R.; et al. Anaesthetic efficacy and postinduction hypotension with remimazolam compared with propofol: A multicentre randomised controlled trial. Anaesthesia 2024.
- Renew, J.R. Is remimazolam the elusive anesthetic on/off switch?. Can J Anesth/J Can Anesth 71, 1057–1061 (2024). https://doi.org/10.1007/s12630-024-02736-y
- “Remimazolam: A New Drug Looking For a Niche.” Manzano, Antoni et al. Journal of Cardiothoracic and Vascular Anesthesia, Volume 38, Issue 9, 1842 – 1844
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2024, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Last year, we turned the spot light on a novel, practice-changing medication, Remimazolam for a two-part series. Today, we are revisiting our earlier discussion in one high yield show.
Before we dive into the episode today, we’d like to recognize Nihon Kohden, a major corporate supporter of APSF. Nihon Kohden has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Nihon Kohden – we wouldn’t be able to do all that we do without you!”
Our featured article is “Remimazolam: Patient Safety Considerations of a Novel, Practice-Changing Drug in Perioperative Medicine” by Arnoley Abcejo and Miguel Teixeira. To follow along with us, head over to APSF.org and click on the Newsletter archives. The fourth one down is Newsletter archives. Then, scroll down until October 2023. From here, scroll down until you get to our featured article today. I will include a link in the show notes as well.
And now, it’s time to return to Episode #175. Here we go:
[Music Interlude]
[Episode #175] “Before we dive into the article, we are going to hear from one of the authors. Here he is now.
[Teixeira] “Hello, my name is Miguel Teixeira and I’m an anesthesiologist and intensivist at the Mayo Clinic in Rochester, Minnesota. Thanks so much for having me.”
[Bechtel] To kick off the show, I asked Teixeira what got him interested in this topic. Let’s take a listen to what he had to say.
[Teixeira] “At first, I heard about Remimazolam from some colleagues at work. I was immediately intrigued by its pharmacokinetics and pharmacodynamics. Fast onset, short acting, reversible. As a neuro-anesthesiologist and intensivist, I knew benzodiazepines as a whole had an appealing profile.
Favorable effects on respiratory drive and hemodynamics, and its effects on neurophysiology, even. Yet I actually rarely used them. Why? Well, as a whole, benzodiazepines had a slower rate of loss of consciousness and a longer context sensitive half-life compared to other available agents. Also, I was concerned about the potential deleterious neurologic recovery side effect profile.
So, with that in mind, together with some colleagues in the Division of Neuro-anesthesia, we started researching Remimazolam’s role specifically as it pertains to neurosurgery and in those patients with neurologic diseases.”
[Bechtel] Now, we’re all excited to learn more about this new medication.
Have you used Remimazolam before? Do you have it available at your institution? Remimazolam is an IV, short-acting, and ultrafast onset benzodiazepine that acts as a potent sedative-hypnotic, anxiolytic, anticonvulsant, and muscle relaxant. The name was designed to remind you of the therapeutic effects of midazolam and the unique metabolism of remifentanil.
Remimazolam has been used for procedural sedation in Asia and Europe since it was first released in China in 2019 for use in gastrointestinal endoscopy. The use has expanded to general anesthesia in Japan and Korea as well as IV sedation in Belgium. In July 2020 in the United States, the FDA approved remimazolam for induction and maintenance of sedation for adults undergoing procedures lasting 30 minutes or less. There are many reported off-label uses as well. Over the past 3 years, this drug has not been acquired by many institutions or used in a large clinical practice.
The authors share the experience at their institution, the Mayo Clinic, which is one of the first major academic centers in the United States to incorporate remimazolam in perioperative and periprocedural practice including over 5,000 patients and over 20,000 doses administered. We are going to take a journey through the literature and the clinical experience at the Mayo Clinic to discuss the unique pharmacokinetics and pharmacodynamics as well as the known limitations, adverse events, and contraindications. The authors also provide key clinical practice implications and help to identify existing knowledge gaps for safe, widespread adoption.
First up, let’s talk about the pharmacology. The mechanism of action is to enhance the gamma-aminobutyric acid type A (GABAA) inhibitory receptor leading to increased frequency of opening of ligand-gated chloride ion channels. Following administration, there is minimal cardiac or respiratory depression. When compared to Midazolam, there is faster onset and dose-dependent sedation and about half the potency for procedural sedation. The sedative effects can be reversed with flumazenil.
Table 1 in the article is a great quick reference guide for remimazolam which includes the pharmacology and dosing. I will include it in the show notes as well. Let’s go through it now. Remimazolam is a benzodiazepine with the following characteristics:
- Sedation time: 11-14 minutes
- Time of peak effect: 3-3.5 minutes following 1 dose and 11-14 minutes following multiple doses
- Half-life elimination: 37-53 min
- Metabolism is esterase dependent.
- Distribution: 0.76-0.98L/kg
- Excretion is via urine.
- Protein-binding is greater than 91%, primarily to albumin.
What all this means is that remimazolam has a relatively high clearance, a small steady-state volume of distribution, shorter elimination half-life, and a short context sensitive half time compared to other benzodiazepines or propofol. This medication is highly bound to protein and metabolized by liver carboxylesterase before being excreted in the urine. Remimazolam is water-soluble. After dilution into a solution, it is painless when injected. Remimazolam is most soluble in slightly acidic solutions and can precipitate in lactated or acetated Ringer’s solution. Check out figure 1 in the article which depicts remimazolam precipitation in plasmalyte. You can administer Remimazolam through y-site co-administration with other common anesthetic medications including remifentanil, fentanyl, dexmedetomidine, midazolam, rocuronium, and vecuronium. The remimazolam approved in the United States is ByFavo which is prepared in a 20mg powder vial which is meant to be drawn up into 8.2ml sterile 0.9% sodium chloride which results in 2.5mg/ml after being reconstituted. The FDA labelling recommends the following:
Inject 2.5-5mg over one-minute followed by supplemental doses of two 1.25-2.5mg doses IV over a 15-second time period after at least two minutes.
The authors share their experience for procedural sedation which includes administration of 2mg IV every 15 seconds as needed with or without analgesic adjuncts such as ketamine or opiates. Induction of general anesthesia involves the administration of a 0.2-0.4mg/kg induction dose followed by 1-2 mg/kg/hr.
There is another great reference in the article, Figure 2, Practical Clinical Considerations. Don’t worry I will include it in the show notes, and we will go through it now.
First, the pharmacodynamics. Following administration of a 0.1mg/kg bolus of remimazolam, onset of sedation is within 60 seconds, maximum plasma concentration occurs within 1-2 minutes, and peak sedation lasts for 1-4 minutes with the patient being fully alert in 10.5 minutes.
Next, pharmacokinetic clearance. There is rapid systemic clearance that is three times faster than midazolam. For bonus points, remember that remimazolam is hydrolysed byCES-1 into inactive metabolite, and severe hepatic dysfunction will reduce clearance by about 38%. There is a low volume of distribution and a short terminal elimination half-life.
Now, let’s do a quick review of route and dosage. Intravenous is clear and painless, but it is incompatible with lactated ringers and safe to administer by y-site with other anesthetics. Intranasal is painful and has a bioavailability of about 50%. Oral route has very poor bioavailability of only 1-2%. For sedation, fixed boluses may be administered in 1-5mg IV every 2 minutes as needed for desired effect. For general anesthesia, induction doses range from 6-12 mg/kg/hr with maintenance rates of 1-2 mg/kg/hr.
We are going to switch our focus from clinical use of remimazolam to discuss the unknown patient safety considerations. This is not a medication with a long track record of use. It is a new medication on the scene. Fortunately, it appears to be a relatively safe medication, but we probably do not know that full impact of this medication on the clinical outcomes after use for specific surgeries or procedures or for specific patient populations. It is so important that any unexpected serious adverse events following remimazolam administration are reported to help improve our understanding of this novel medication in clinical practice…and to help keep patients safe. The authors provide a list of important patient safety considerations or questions that we need to figure out going forward. Let’s review it now.
- Recovery in neurologically vulnerable patients:
- We know that benzodiazepine may increase the risk for perioperative delirium and may need to be avoided for neurologically vulnerable patients, especially the elderly. Postoperative delirium following remimazolam administration only has not been extensively studied and the results may not be generalizable to larger populations or procedure types. At this time, we just do not know what the relationship is between remimazolam administration and long-term postoperative neurocognitive disorder.
- Check out the most recent literature on remimazolam published this year in the journal of neurosurgical anesthesiology by Teixeira and colleagues. Don’t worry, I will include a link in the show notes as well.
- Adverse reactions in specific patient populations and surgical subtypes:
- The pharmacokinetic properties of remimazolam are not significantly altered in elderly patients or patients with higher ASA scores. Keep in mind that according to the FDA recommendations, you may need a slight decreased dose for these patients as well as a reduced dose for patients with severe hepatic impairment as evidenced by a child-Pugh score greater than or equal to 10 due to the concern or decreased drug clearance. For remimazolam, you do no need to change the dose for patients with severe kidney disease. Currently, there are no recommendations for administration for pediatrics, but you can find off-label case reports of remimazolam as an adjunct for general anesthesia in the literature. There are also no case reports of the use of this medication in pregnant patients. If you take care of pediatric patients, we hope that you will check out the June 2023 article in the Journal of Clinical Medicine, “Remimazolam as an Adjunct to General Anesthesia in Children: Adverse Events and Outcomes in a Large Cohort of 418 Cases” by Kimoto and colleagues.
- Spoiler alert the authors of that study conclude that remimazolam administration to pediatric patients as an adjunct to general anesthesia may be associated with hemodynamic variability which may require treatment as well as a rapid return to responsiveness and ability to meet discharge criteria. The authors leave us with a call to action that large, multicenter trials are needed to learn more about remimazolam administration safety for pediatric patients.
[Music Interlude]
We are going to fast-forward to Episode #176 and continue the conversation on Remimazolam so stay tuned.
[Episode #176] “This week, we are going to hear from the other author of the article. Here he is now.
[Abcejo] “Hello, my name is Arnie Abcejo. I am an anesthesiologist at Mayo Clinic, Rochester, the division chair of neuro-anesthesiology and radiology and the APSF website medical director.”
[Bechtel] To kick off the show today, I asked Abcejo, why he wrote this article. Let’s take a listen to what he had to say.
[Abcejo] “We wrote this article for a couple reasons. First, anecdotally, our group has been asked by many other large and small private and academic practices across the country on our use, why we use it, how we use it, and how it’s made an impact on our large practice.
We wanted to share that information more broadly with a venue like the APSF. Secondly, there are patient safety considerations that we need to be aware of in this drug, and because so, it behaves so much unlike midazolam. Thirdly, a lot of information in GI and pulmonology, and not necessarily from anesthesia.
I think as the experts in perioperative patient safety, we should have a leadership role in what makes this drug safe and how we should use it. I think what, uh, I’m really astounded with remimazolam is its impact on our practice, um, here at Mayo Clinic.
Since we first launched this trial use of this drug in 2021, we’ve administered the drug safely and successfully in thousands of patients. And in many ways, it’s become the standard of care for some specific procedures for sedation. To have an impact on a large quaternary system like ours, I’ve never really seen a drug like that before.
Uh, before, and I’m absolutely sure this drug will have an impact on not only perioperative medicine, but also health care as a whole.”
[Bechtel] Thank you so much to Abcejo for contributing to the show today. We are so excited to learn more about remimazolam and see what kind of impact this medication will have in the future.
And now it’s time to jump back into the article. We left off last week by discussing important patient safety considerations associated with remimazolam use that we need to evaluate going forward. We are going to pick up right there.
We still need to figure out the administration and practice guided by non-anesthesia professionals. Administration of midazolam by periprocedural nursing staff is very common. At this time, there are gastrointestinal endoscopic studies that report the safe use of remimazolam by non-anesthesia professionals. The authors’ experience at the Mayo clinic has been that changing from a midazolam sedative nursing practice to a remimazolam sedative nursing practice takes time, training, and cultural shifts and this is especially important to help ensure patient safety.
Another consideration is the cost and access. Remimazolam is more expensive than other common sedative medications including midazolam and propofol. This increased cost may be balanced by the faster recovery times that may facilitate increased procedural efficiency.
We are going to shift gears to talk about the adverse reactions and contraindications for remimazolam use. Remimazolam appears to be a safe medication with mild and short-lived adverse reactions that are reversed by a single dose of flumazenil. Remember, remimazolam has a short context-sensitive half-life, but you still need to be careful to ensure adequate reversal in patients receiving a prolonged infusion, with significant liver disease, and with co-administration with opioids. Even though re-sedation from remimazolam after reversal is unlikely, this has been reported in the literature.
Let’s review the common adverse reactions following remimazolam administration.
- Heart rate and blood pressure changes
- Body movement
- Nausea
- Dizziness
- Headaches
Keep in mind that adverse reactions are less likely to occur than following propofol administration and at a similar rate to midazolam. Co-administration of remimazolam with other central nervous system depressants including opioids may lead to significant respiratory depression. Remain vigilant for anaphylaxis which has been reported in the literature. Contraindications to remimazolam administration includes patients with a known severe hypersensitivity reaction to Dextran 40. More studies are needed to evaluate the risk of postoperative nausea and vomiting and remimazolam administration. There is likely a decreased risk compared to volatile anesthetics, but not when compared to propofol.
Now is the moment you have all been waiting for, a deep dive into the clinical practice implications. The authors report that since its introduction at their institution, remimazolam was quickly adopted in almost every area of practice especially in clinical areas with complex patients and procedures. Let’s take a look at the specific clinical areas.
First up, for patients with complex cardiovascular or hemodynamically unstable patients remimazolam has limited impact on respiratory depression, systemic vascular tone, and inotropic, dromotropic, and chronotropic function. Thus, remimazolam may be used for patients undergoing cardiac catheterization, especially cardioversions, and during cardiac surgery and trauma cases in patients with limited cardiopulmonary reserve.
Second, remimazolam may be used for non-operating room anesthesia or NORA procedures. Remimazolam may be used for patients undergoing GI and Pulmonary Endoscopic Procedures. Studies have revealed a comparable efficacy for procedural sedation with less hemodynamic variability, painless IV injection, decreased postoperative nausea and vomiting, and a rapid return to baseline neurological function. Wow, that all sounds great! For patients undergoing interventional radiology procedures, remimazolam may be used to provide sedation, amnesia, and anxiolysis. The new medication may have a big impact in this space since these patients may be sicker with multiple comorbidities, require deeper levels of sedation, and are too unstable to open surgical procedures and these procedures often have limited, intermittent periods of stimulation. Patients, such as those with claustrophobia, musculoskeletal discomfort, and tremors, who need sedation when undergoing magnetic resonance imaging may benefit from remimazolam administration. Remimazolam may also be used with dexmedetomidine to provide monitored anesthesia care for MRI. Here are some good examples, patients with central spinal cord stenosis may be safely sedated with intermittent remimazolam boluses to obtain the imaging with intermittent neurological exams to monitor for permanent spinal cord ischemia. Small doses may be given to patients for anxiolysis while maintaining a patent airway to complete a brain MRI. The authors point out that the Mayo Clinic does not formally have nurses performing sedation with remimazolam.
Finally, there appears to be a role during neurosurgical procedures since it provides rapid amnestic sedation and anxiolysis which may be quickly followed by a meaningful neurologic exam. The authors report using this medication for awake craniotomies during pin placement, local anesthetic administration, urethral catheter placement, and surgical incision.
The authors’ experience with remimazolam is that it will likely have a big impact on a variety of clinical situations given the attractive pharmacokinetics, relative respiratory and hemodynamic safety profile, and rapid reversal with likely expansion into nurse sedation practice as well as outpatient and ambulatory settings going forward. The authors leave us with this call to action:
“Anesthesia professionals have a unique opportunity to identify patient safety practice guidelines, clinical guardrails, and safety algorithms for remimazolam. More large patient cohort safety data are forthcoming to truly delineate its safety profile compared to the other commonly used sedatives in the anesthesia professionals’ arsenal.”
[Bechtel] We hope you enjoyed this revisited show all about Remimazolam. Are you using this medication as part of your anesthesia practice? If you get a chance, we hope that you will check out the citations in the show notes for new articles that evaluated Remimazolam and were published in the past year. We are still learning more about this novel anesthetic medication.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today. We’ll be back next week to talk about an all-new article from the October 2024 APSF Newsletter.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2024, The Anesthesia Patient Safety Foundation
