Episode #181 Keeping Patients with Food Bolus Impaction or Foreign Object Ingestion Safe During Anesthesia Care, PART 2
December 20, 2023
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is “Preoperative Evaluation and Selection of Anesthesia Technique for Endoscopic Treatment of a Patient with Food Bolus Impaction or Foreign Object Ingestion” by George Tewfik; Govind Rangrass; James Dierkes; and Uma Munnur.
Special thanks to George Tewfik for contributing to the article today.
Here is Figure 1 from the article! You may want to print this out for your endoscopy suite or hang it up in your call room or save the image on your phone for quick reference:
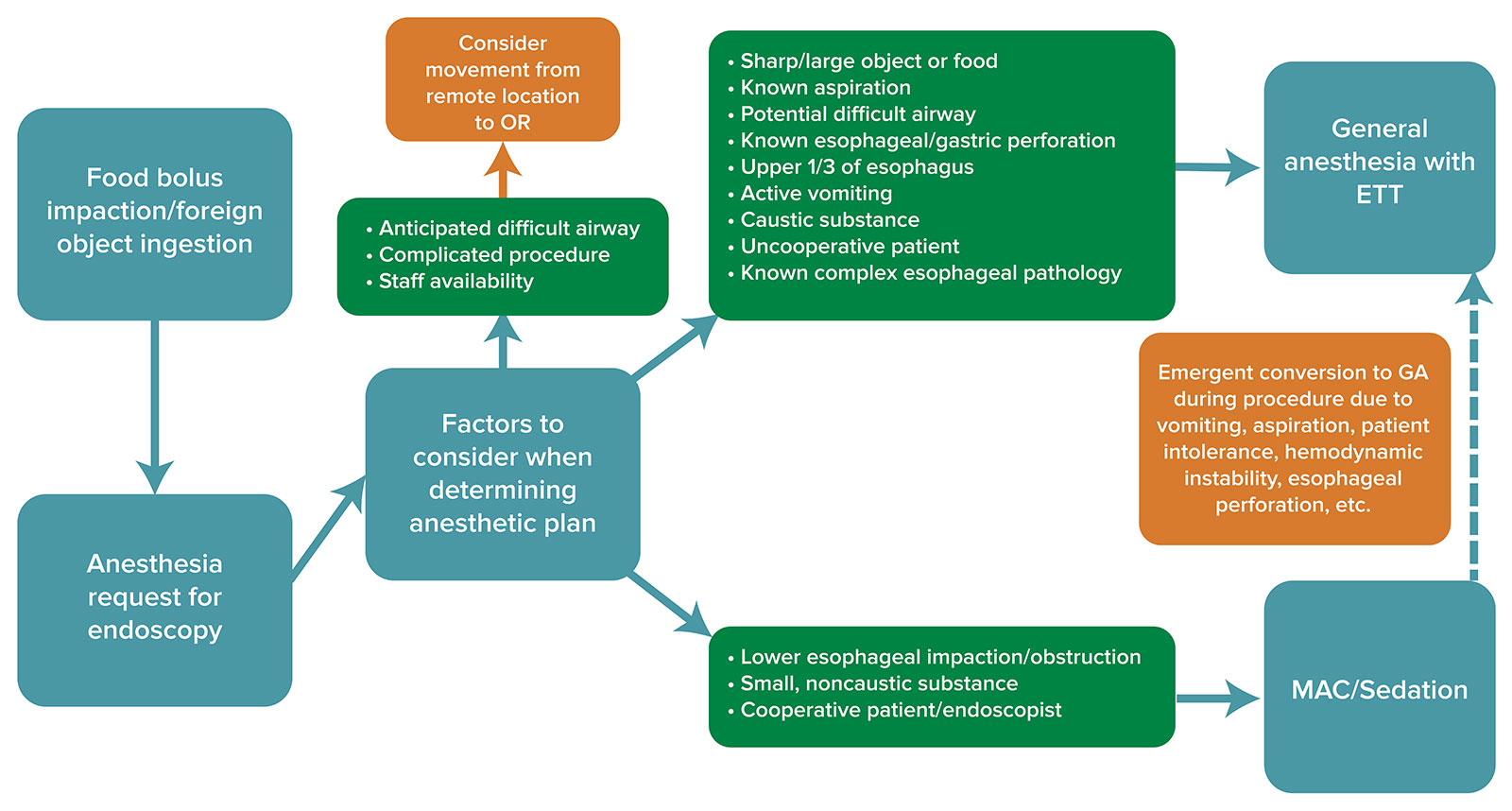
Figure 1: Algorithm for decision-making regarding the anesthetic care of a patient presenting for endoscopy with either food bolus impaction or foreign object ingestion. Consideration should be given to factors such as airway exam, procedure type, staffing, and logistics to determine anesthetic technique and proper setting for procedure. MAC: monitored anesthesia care, GA: general anesthesia, ETT: endotracheal tube
Important considerations for providing safe anesthetic care for patients undergoing endoscopic retrieval of food bolus or foreign body include the following:
- There is no uniform anesthetic approach.
- Effective communication with the patient, endoscopist, and ancillary staff is vital.
- Proper planning is necessary especially when these procedures are performed in a remote location.
- Make sure you have a backup plan in place for complications including failed sedation, aspiration or airway obstruction or procedural complications that may require emergent surgical intervention.
Do you want to learn more about low-flow anesthesia so that you can deliver safe & effective patient care while decreasing cost & environmental pollution. If this is something that you want to make part of your safe anesthesia practice, head over the APSF low-flow course. The course is free of charge to all anesthesia professionals, but a guest login is required for non-ASA members. There are continuing education credits available for physicians, nurses and anesthesia assistants. For physicians enrolled in the MOCA process, the CME credits are patient safety eligible. Check it out here: https://www.apsf.org/apsf-technology-education-initiative/low-flow-anesthesia/
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2023, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. Last week, we started the conversation about preoperative evaluation and choice of anesthetic technique for patients presenting with food bolus impaction or foreign body ingestion for endoscopic retrieval. Have you provided anesthesia care for this procedure recently? Did you select general anesthesia with an endotracheal tube or monitored anesthesia care and sedation? It is so important to evaluate the patient carefully, weigh the risks and benefits, and communicate with the proceduralist before deciding on an anesthetic technique. We are going to continue the conversation today, so don’t turn the dial.
Before we dive into the episode today, we’d like to recognize GE Healthcare, a major corporate supporter of APSF. GE Healthcare has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, GE Healthcare – we wouldn’t be able to do all that we do without you!”
Our featured article today is, once again, “Preoperative Evaluation and Selection of Anesthesia Technique for Endoscopic Treatment of a Patient with Food Bolus Impaction or Foreign Object Ingestion” by George Tewfik and colleagues. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue. From here, scroll down until you get to our featured article today. I will include a link in the show notes as well.
Before we get into the article, we are going to review a helpful tool for selecting a safe anesthetic technique for patients presenting with food bolus impaction or foreign body ingestion who need to undergo endoscopic retrieval or manipulation. Check out Figure 1 in the article! You may want to print this out for your endoscopy suite or hang it up in your call room or save the image on your phone for quick reference. We are going to go through it now!
The first box is food bolus impaction or foreign object ingestion followed by the request for anesthesia services. From here, you can move on to the box labeled, Factors to consider when determining the anesthetic plan. Then, the first arrow points to a green box with the following points:
- Anticipated difficult airway.
- Complicated procedure
- Staff availability
If this describes the situation, then it is important to consider performing the procedure in the operating room rather than in a remote endoscopy location.
Next, you can follow the second arrow that points to a large box with the following considerations:
- Sharp or large object or food
- Known aspiration.
- Potential difficult airway
- Known esophageal or gastric perforation.
- Upper 1/3 of esophagus
- Active vomiting
- Caustic substance
- Uncooperative or combative patients or pediatric patients
- Known complex esophageal pathology.
If these conditions are present, then please proceed to the General Anesthesia with Endotracheal Tube box.
There’s one more arrow that you can follow to a third green box with the following considerations:
- Lower esophageal impaction/obstruction
- Small non-caustic substance
- Cooperative patient and endoscopist
From here, you may proceed to the MAC or Sedation option for anesthesia care as long as you maintain the ability to provide a secure airway if needed for an emergency. Emergent conversion to general anesthesia may be required due to vomiting, aspiration, patient intolerance, hemodynamic instability, or esophageal perforation.
Don’t worry, you can find Figure 1 in the show notes or in the article. This algorithm may be helpful for decision-making regarding the anesthetic care of a patient presenting for endoscopy with either food bolus impaction or foreign object ingestion.
Another decision point may be related to the surgical technique. Have you seen cap-assisted endoscopy? This is where there is a cap fitted to the end of the scope to help depress mucosal folds and improve visualization leading to increased rate of treatment success and shorter procedure time for patients with food bolus impaction or foreign body ingestion, and this may lead anesthesia professionals to perform sedation for the procedure instead of a general anesthetic with an endotracheal tube. Another time sedation may be used is for non-urgent endoscopies for patients with ingested medium-sized blunt objects. These cases may be delayed for up to 72 hours from the time of initial ingestion. Endoscopists may use an overtube with the endoscope inserted through this device. This may help decrease the risk for aspiration by creating an occlusive conduit from the esophagus to outside the oral cavity and decrease mucosa damage from trauma.
There may be some implications for the choice of anesthetic technique depending on the logistics of the treatment facility. These procedures may be performed in the emergency room, endoscopy suite, hospital bed, or another remote location far from the operating rooms. It is important to consider the following factors:
- Space constraints
- Difficult patient access
- Poor lighting
- Limited monitoring
- Lack of advanced airway equipment
- Lack of experienced ancillary staff
- Poor communication with personnel involved in patient care.
We know that emergency airway management may be difficult outside of the operating room and there is an increased risk for adverse events. It is important to advocate for patients with anatomic variants, poor functional reserve, and high risk for aspiration to be moved to the operating room for a general anesthetic with endotracheal tube for these procedures. Remember, if you find yourself in a remote endoscopy suite, safe anesthesia care requires adequate monitoring, appropriate devices for delivering anesthetic agents, ability to oxygenate and ventilate, and understanding of the surgical procedure and the related risks.
Now, it is time to move on to the next section…Special Safety Considerations. First up, let’s talk about talking or rather communication. Keeping patients safe during endoscopy for retrieval of food bolus or foreign object requires effective communication with the following people:
- Proceduralist
- Patient
- Family members
- Nursing staff
- Technologists
- And administrative personnel.
Communication is vital to ensure timely care, confirm available resources, coordinate with perioperative staff and the patient’s primary care service in the facility. If you decide to perform MAC for endoscopic retrieval in a remote location, it is necessary to confirm that equipment and personnel are available to convert to general anesthesia if required by the patient’s medical condition or the procedure. Before induction, make sure that you have advanced airway equipment available including a video laryngoscope, fiberoptic bronchoscope, and intubating LMAs in case of an emergency or an unanticipated difficult airway.
We made it to the end of the case…whew! It’s time to talk about postoperative care. This is another time when anesthesia professionals must remain vigilant since patients are at risk for esophageal or gastric perforation, gastrointestinal bleeding, and aspiration. Keeping patients safe requires careful monitoring by qualified personnel for signs of hypoxemia, wheezing, and hemodynamic instability. Additional help from ancillary services, such as thoracic surgery, may be required in case of serious complications such as esophageal perforation leading to pneumomediastinum or esophageal rupture. Patients who develop complications may require postoperative care in the critical care unit as well.
We made it to the end of the article. Important considerations for providing safe anesthetic care for patients undergoing endoscopic retrieval of food bolus or foreign body include the following:
- There is no uniform anesthetic approach.
- Effective communication with the patient, endoscopist, and ancillary staff is vital.
- Proper planning is necessary especially when these procedures are performed in a remote location.
- Make sure you have a backup plan in place for complications including failed sedation, aspiration or airway obstruction or procedural complications that may require emergent surgical intervention.
Before we wrap up for today, we are going to hear from Tewfik again. I also asked him, “What do you envision for the future with regards to this area of anesthesia care? Let’s take a listen to his response.
[Tewfik] “As more and more surgical procedures and anesthetics are performed outside of the operating room; we envision additional research being conducted regarding safe perioperative care in remote locations.
In particular, there will likely be an increasing body of work regarding safe anesthesia for complex endoscopic procedures, such as that done for food impaction, foreign body retrieval, in addition to ERCPs and weight loss procedures. Improved systems including availability of equipment, support services, and advanced recovery room nursing will be required as the acuity of patients increases outside of the OR.
However, with appropriate planning and anticipation of patient care, anesthesia may be safely performed for advanced endoscopic procedures in both elective and emerging cases such as those involving food impaction and foreign bodies.”
[Bechtel] Thank you so much to Tewfik for contributing to the show today and highlighting important considerations for keeping patients safe during anesthesia care for these challenging cases.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
If you have been listening to this podcast, then you already know that low-flow anesthesia can deliver safe & effective patient care while decreasing cost & environmental pollution. If this is something that you want to make part of your safe anesthesia practice, head over the APSF low-flow course. Check out the link in the show notes or head over to our website, apsf.org. Then, click on the Patient Safety Resources heading, 6th one down is APSF Technology Education initiative, then click on Low Flow Anesthesia. The course is free of charge to all anesthesia professionals, but a guest login is required for non-ASA members. There are continuing education credits available for physicians, nurses and anesthesia assistants. For physicians enrolled in the MOCA process, the CME credits are patient safety eligible.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2023, The Anesthesia Patient Safety Foundation
