Episode #180 Anesthetic Considerations for Patients with Food Bolus Impaction or Foreign Object Ingestion
December 13, 2023
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is “Preoperative Evaluation and Selection of Anesthesia Technique for Endoscopic Treatment of a Patient with Food Bolus Impaction or Foreign Object Ingestion” by George Tewfik; Govind Rangrass; James Dierkes; and Uma Munnur.
Special thanks to George Tewfik for contributing to the article today.
Here are the citations that we talked about on the show today:
- Cha MH, Sandooja R, Khalid S, et al. Complication rates in emergent endoscopy for foreign bodies under different sedation modalities: a large single-center retrospective review.World J Gastrointest Endosc. 2021;13:45–55. PMID: 33623639
- Geng C, Li X, Luo R, et al. Endoscopic management of foreign bodies in the upper gastrointestinal tract: a retrospective study of 1294 cases. Scand J Gastroenterol. 2017;52:1286–1291. PMID: 28691540
Here is Figure 1 from the article. This is a good resource for anesthesia professionals who may be taking care of patients undergoing this endoscopic procedure.
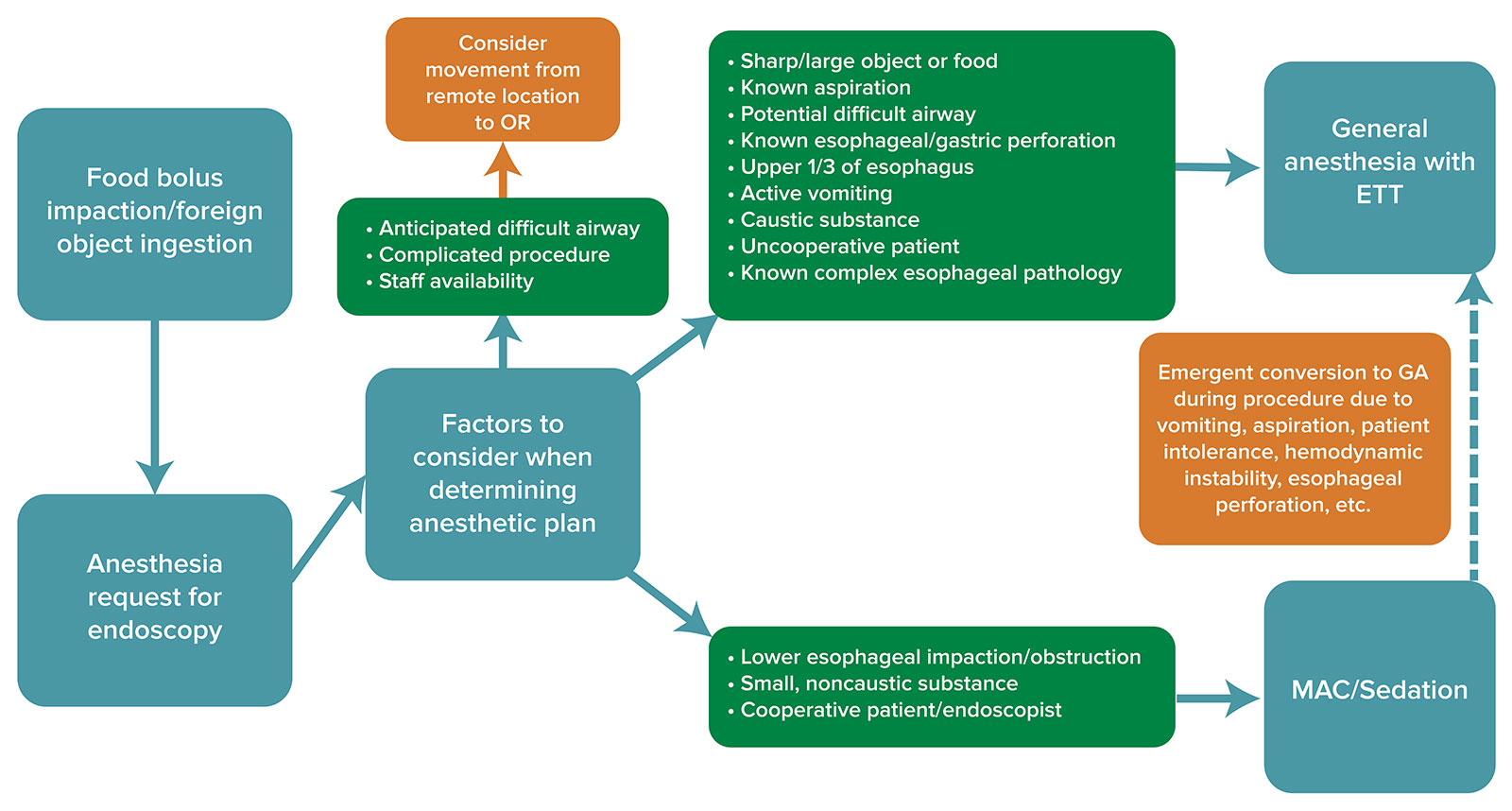
Figure 1: Algorithm for decision-making regarding the anesthetic care of a patient presenting for endoscopy with either food bolus impaction or foreign object ingestion. Consideration should be given to factors such as airway exam, procedure type, staffing, and logistics to determine anesthetic technique and proper setting for procedure. MAC: monitored anesthesia care, GA: general anesthesia, ETT: endotracheal tube
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2023, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. It may be December already, but there are still some excellent articles from the October 2023 APSF Newsletter. Today, we are talking about a fairly common procedure where the choice for anesthetic technique is often debated.
Before we dive into the episode today, we’d like to recognize Fresenius Kabi, a major corporate supporter of APSF. Fresenius Kabi has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Fresenius Kabi – we wouldn’t be able to do all that we do without you!”
Our featured article today is “Preoperative Evaluation and Selection of Anesthesia Technique for Endoscopic Treatment of a Patient with Food Bolus Impaction or Foreign Object Ingestion” by George Tewfik and colleagues. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue. From here, scroll down until you get to our featured article today. I will include a link in the show notes as well.
Before we get into the article, we are going to hear from the author. Let’s take a listen.
[Tewfik] “Hi, my name is George Tewfik, and I’m an associate professor in anesthesiology at Rutgers New Jersey Medical School in Newark, New Jersey.”
[Bechtel] To kick off the show today, I asked Tewfik why he is so passionate about this topic. Here is his response.
[Tewfik] “Our team wrote this article because anesthesia for an endoscopic procedure to treat food bolus impaction or foreign body ingestion presents a unique set of challenges for an anesthesia team.
Not only are these patients at high risk for aspiration or gastrointestinal complications such as bleeding or perforation, but these procedures are also often performed in remote locations without the support found in an operating room. Our article reviews such important considerations as clinical presentation, underlying conditions, proposed surgical approach, and logistics when one approaches the anesthesia for this patient population.”
[Bechtel] Thank you so much to Tewfik for providing exclusive content for the show today. We are so excited to get into this article and don’t worry, we are going to hear from Tewfik again.
And now it’s time for the article. Let’s start with some background. Our discussion today is going to focus on providing anesthesia care for patients with food bolus impaction and foreign body ingestion who require urgent endoscopy procedures with either a push or retrieval technique. There may be significant complications during or after this procedure including gastrointestinal perforation, bleeding, or ulceration. For pediatric patients, the most common objects ingested include coins, toys, magnets, and batteries. Check out episodes #96 and 97 for more information about keeping pediatric patients safe following button battery ingestion. In adults, the most common cause of food bolus impaction is bone or meat bolus. Foreign body ingestions are more likely to occur in children, psychiatric patients, and prisoners while food bolus impaction is more likely to occur in elderly male patients with a history of esophageal pathology, such as esophagitis, esophageal strictures, and hiatal hernias.
The majority of food boluses are found in the lowest third of the esophagus, and this location is related to the associated complications which may include esophageal erosion, mucosal damage, foreign body sensation, odynophagia, and sialorrhea. Ingested foreign bodies are usually found in the upper two-thirds of the esophagus and may be associated with inability to clear secretions and injury to the airway. Patients may be at risk for life-threatening complications depending on the ingested food or object, the location, any underlying pathology, and time to treatment.
So, how can we retrieval or move the ingested food bolus or foreign body to relieve the obstruction? Patients who undergo endoscopic retrieval or manipulation to relieve an acute obstruction are more likely to have successful removal, lower rates of minor complications, and decreased need for surgery or hospitalization. Keep in mind that the rate of complications increases with longer duration of the obstruction and with increased size or type of the foreign body. The authors provide the example of a patient who presents following sharp pointed food impaction and is at high risk for esophageal perforation. This is the scenario for early endoscopic intervention.
Patient presentation may include dysphagia, odynophagia, vomiting, or feelings of choking and gagging. Impaction or ingestion may lead to obstruction which may cause airway compromise, failure to handle secretions, and even death.
We are going to review the tools that may be used during endoscopy by the proceduralist to retrieve the ingested material including baskets, retrieval forceps, polypectomy, snares, and nets. These procedures may be performed with flexible endoscopy which may not require anesthesia or rigid endoscopy.
We have so much more to talk about when it comes to keeping patients safe during these procedures. So, let’s turn our attention to anesthetic considerations for endoscopy. There are different standards for sedation and anesthetic practices depending on different institutions and legal jurisdictions. Sedation may be administered by anesthesia professionals or non-anesthesia personnel including nurses and gastroenterologists. Medication options may include IV sedative-hypnotic medications, benzodiazepines, and opioids. In 2018, the American Society for Gastrointestinal Endoscopy published guidelines for the standards of care for patients undergoing endoscopy procedures who are supervised by interventional gastroenterologists. Sedation may be provided by non-anesthesia professionals with topical anesthetics and minimal or no IV medications to moderate sedation with propofol and other IV medications. This may only be in locations where non-anesthesia professional administered propofol is permitted. These guidelines report that when sedation for endoscopy is provided by anesthesia professionals, there is higher patient satisfaction, decreased distractions for the endoscopist, increased procedure volume in the endoscopy unit since there is shorter sedation times with faster recovery. As a result, anesthesia professionals are often requested for endoscopic procedures and today, we are focusing on endoscopic retrieval of food bolus or foreign body.
When you are called to the endoscopy suite for food bolus impaction or foreign body ingestion, what is your choice for the anesthetic? We still don’t know the optimal anesthetic technique for these procedures. It is really important to weigh the risks and benefits. There is a risk for aspiration during endoscopic manipulation which may point to general anesthesia with an endotracheal tube to protect the airway and keep patients safe. However, monitored anesthesia care and sedation is often used and studies have not revealed a superior approach.
Let’s take a look at the 2021 study by Cha and colleagues, “Complication rates in emergent endoscopy for foreign bodies under different sedation modalities: A large single-center retrospective review.” This was a retrospective chart review of over 900 endoscopy cases with non-anesthesia provided conscious sedation, and anesthesia professional provided MAC and GA with no difference in adverse events. The most common complications were related to the surgery including mucosal laceration and bleeding with rare aspiration events. In this study, 5.6% of patients receiving conscious sedation required conversion to anesthesia-professional MAC or GA. Another study of over 1000 cases also found no difference in adverse events for patients who received general anesthesia compared to topical pharyngeal anesthesia. This is reassuring that there are options for safe anesthesia care. I will include the citations in the show notes as well.
Preoperative evaluation prior to the endoscopy procedure is vital to keep patients safe. It is important to determine the presence or absence of a full stomach, and this may be difficult for patients with food bolus impaction or foreign body ingestions. There is a higher risk for aspiration when there is increased volume in the stomach, failure of the lower esophageal sphincter to prevent retrograde movement of gastric contents and absent of blunted upper airway reflexes. These risks may all be present during endoscopic retrieval procedures which increases the risk for aspiration. Thus, general anesthesia with an endotracheal tube may be the safest option for patients undergoing these procedures. The authors state that “great care should be taken to consider deviation from this choice of anesthetic.” It is vital to complete a physical examination and history with assessment of the gastrointestinal status and discuss the case with the proceduralist whenever considering other anesthetic options and make sure that you have a way to convert to a secure airway with an endotracheal tube if needed.
Okay and now it’s time to talk developing a safe anesthesia plan for patients undergoing endoscopic retrieval following food bolus impaction or foreign body ingestion. Check out Figure 1 in the article and we are going to go through it now. You may want to print this and make sure that it is available wherever anesthesia professionals are providing anesthesia care during these procedures.
The first box is food bolus impaction or foreign object ingestion followed by the request for anesthesia services and then you move on to the box labeled factors to consider when determining the anesthetic plan. From here, the first arrow points to a green box with the following points:
- Anticipated difficult airway.
- Complicated procedure
- Staff availability
If this describes the situation, then it is important to consider movement away from a remote location to the operating room.
The second arrow points to a large box with the following considerations:
- Sharp or large object or food
- Known aspiration.
- Potential difficult airway
- Known esophageal or gastric perforation.
- Upper 1/3 of esophagus
- Active vomiting
- Caustic substance
- Uncooperative or combative patients or pediatric patients
- Known complex esophageal pathology.
If these conditions are present, then please proceed to the General Anesthesia with Endotracheal Tube box.
There’s one more arrow pointing to a third green box with the following considerations:
- Lower esophageal impaction/obstruction
- Small non-caustic substance
- Cooperative patient and endoscopist
From here, you may proceed to the MAC or Sedation option for anesthesia care as long as you maintain the ability to provide a secure airway if needed for an emergency. Emergent conversion to general anesthesia may be required due to vomiting, aspiration, patient intolerance, hemodynamic instability, or esophageal perforation.
Don’t worry, I will include Figure 1 in the show notes as well for an algorithm for decision-making regarding the anesthetic care of a patient presenting for endoscopy with either food bolus impaction or foreign object ingestion.
Before we wrap up for today, let’s review the different options for anesthesia care again.
Patients or procedures with the following characteristics are more likely to require general anesthetic with an endotracheal tube and at times as additional resources including equipment and personnel or movement to the operating room for the procedure.
- Obstruction or impaction in the proximal esophagus
- Technically difficult retrieval or anticipated longer procedure duration.
- Ingestion with caustic material
- Large or sharp foreign bodies
- Pediatric or combative patients
- History of abnormal esophageal or gastric anatomy
- Active or recent nausea and vomiting.
- Morbidly obese patients
- Anticipated difficult airway.
Mac or sedation may be provided for patients and procedures with the following characteristics:
- Suspected, but not confirmed ingestion.
- Foreign body in the distal esophagus
- Patients with little or no comorbidities
- No recent vomiting
- Small-sized object or food bolus
- Dull object
- Good patient compliance and acceptance of sedation plan
- Provider and patient preference
There is still so much more to talk about when it comes to considerations related to the surgical technique and treatment facility as well as special safety considerations related to communication and postoperative care. Plus, we are going to hear from Tewfik again, so we hope that you will join us again next week.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
We hope that you will tell your colleagues about the APSF and this podcast as we work to spread the word about improving anesthesia patient safety. For more anesthesia patient safety tweets and posts, please follow us and like us on Facebook, twitter, Instagram, and LinkedIn. We also have a YouTube Channel where you can listen to this podcast, catch up on the APSF Stoelting Conference lectures, and review the APSF Safety Videos.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2023, The Anesthesia Patient Safety Foundation
