Episode #166 Keeping Patients Safe with the Brand New Practice Guidelines for Neuromuscular Blockade
September 5, 2023
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Today, we are focusing on quantitative monitors for neuromuscular blockade with updated practice guidelines to help keep patients safe. Our featured article is “New Practice Guidelines for Neuromuscular Blockade” by Connie Chung, Joseph W. Szokol, Wade A. Weigel, and Stephan R. Thilen.
This is the citation for the new practice guidelines:
- Thilen SR, Weigel WA, Todd MM, et al. 2023 American Society of Anesthesiologists practice guidelines for monitoring and antagonism of neuromuscular blockade: a report by the American Society of Anesthesiologists Task Force on Neuromuscular Blockade. Anesthesiology. 2023; 138:13–41. PMID: 36520073
Here’s the big takeaway from the new guidelines: “Quantitative monitoring of neuromuscular blockade is recommended at the adductor pollicis muscle to confirm TOF ratio greater than or equal to 0.9 before extubation, accompanied by the use of Sugammadex or neostigmine for the antagonism of blockade.”
Check out this article that we talked about on the show today.
- Naguib M, Brull SJ, Hunter JM, et al. Anesthesiologists’ overconfidence in their perceived knowledge of neuromuscular monitoring and its relevance to all aspects of medical practice: an international survey. Anesth Analg. 2019;128:1118–1126. PMID: 31094776
Check out the two supplemental tables for more information about the different quantitative neuromuscular monitors that are available.
- Supplemental Table 24 (Note: link downloads a Word doc), https://links.lww.com/ALN/C928
- Supplemental Table 26 (Note: link downloads a Word doc), https://links.lww.com/ALN/C928
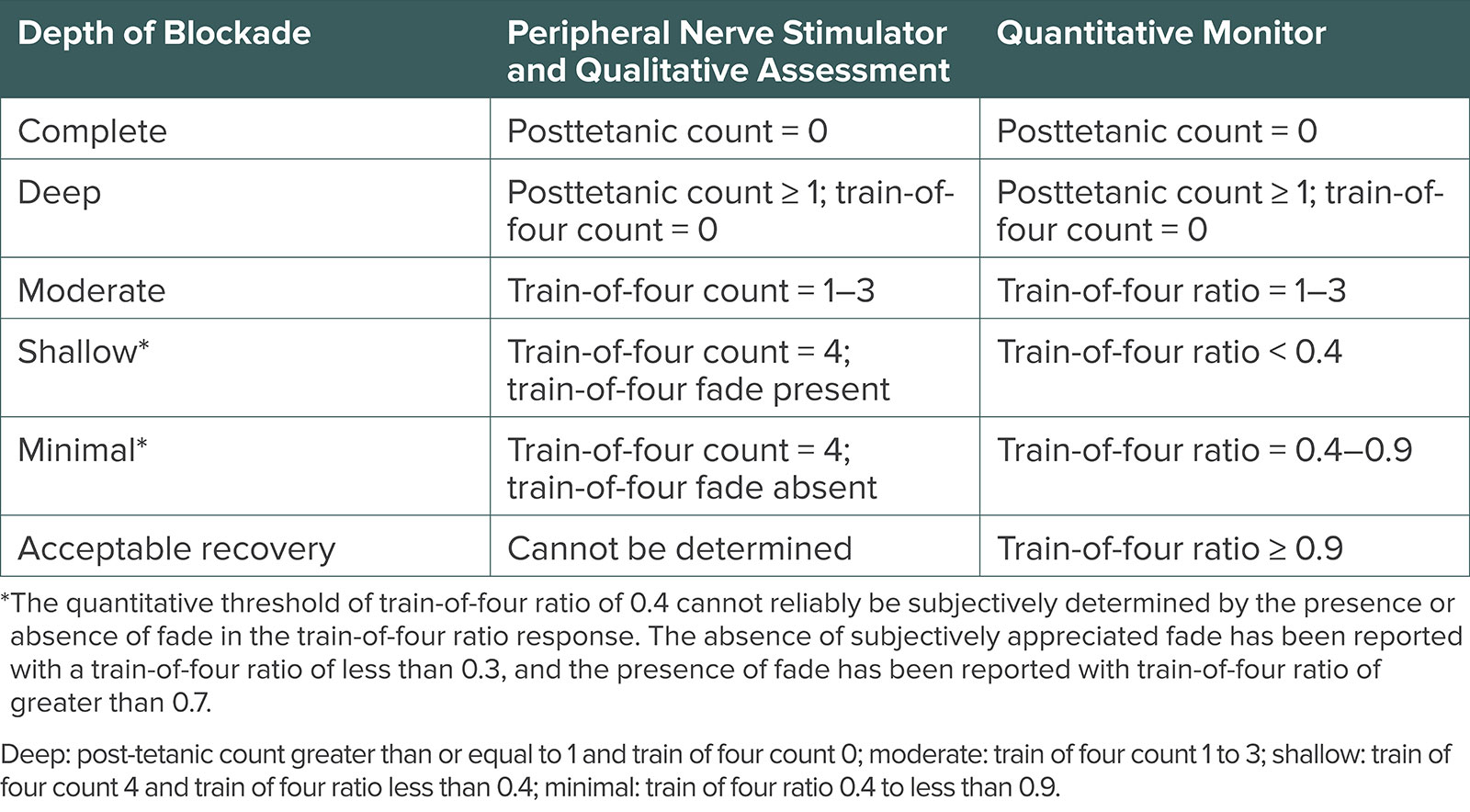
Table 1: Depths of Neuromuscular Blockade by Quantitative and Qualitative Measurement.
Here are all 8 new practice guidelines:
- “When neuromuscular blocking drugs are administered, we recommend against clinical assessment alone to avoid residual neuromuscular blockade, due to the insensitivity of the assessment.1
- We recommend quantitative monitoring over qualitative assessment to avoid residual neuromuscular blockade.
- When using quantitative monitoring, we recommend confirming a train of four ratio greater than or equal to 0.9 before extubation.
- We recommend using the adductor pollicismuscle for neuromuscular monitoring.
- We recommend against using eye muscles for neuromuscular monitoring.
- We recommend Sugammadex over neostigmine at deep, moderate, and shallow depths of neuromuscular blockade induced by rocuronium or vecuronium, to avoid residual neuromuscular blockade.
- We suggest neostigmine as a reasonable alternative to Sugammadex at minimal depth of neuromuscular blockade.
- To avoid residual neuromuscular blockade when atracurium or Cisatracurium are administered and qualitative assessment is used, we suggest antagonism with neostigmine at minimal neuromuscular blockade depth. In the absence of quantitative monitoring, at least 10 minutes should elapse from antagonism to extubation. When quantitative monitoring is utilized, extubation can be done as soon as a train of four ratio greater than or equal to 0.9 is confirmed before extubation.”
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2023, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We are returning to the June 2023 APSF Newsletter today to talk about Neuromuscular Blockade. Residual muscle weakness is a big threat to anesthesia patient safety, and it is important to keep patients safe with appropriate use, monitoring, and reversal.
Before we dive into the episode today, we’d like to recognize GE Healthcare, a major corporate supporter of APSF. GE Healthcare has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, GE Healthcare – we wouldn’t be able to do all that we do without you!”
Historically monitoring neuromuscular blockade involved qualitative monitors for the 5 second head lift or fade on a twitch monitor. Today, we are focusing on quantitative monitors for neuromuscular blockade with updated practice guidelines to help keep patients safe. Our featured article is “New Practice Guidelines for Neuromuscular Blockade” by Connie Chung and colleagues. To follow along with us, head over to APSF.org and click on the newsletter heading. First one down is the current issue. Then scroll down until you get to our featured article today. I will include a link in the show notes as well.
Let’s start with some background information about these guidelines. The American Society of Anesthesiologists Committee on Practice Parameters created a task force to develop neuromuscular blockade guidelines with the goal to improve patient safety and satisfaction. Co-chairs Stephan Thilen and Wade Weigel led the task force to develop the 2023 ASA Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade which we are going to review on the show today. These practice guidelines come with the following disclaimer that I am going to read now:
“ASA practice guidelines aim to improve patient care, safety, and outcomes by providing up-to-date information for patient care. Practice guidelines are subject to revision as warranted by the evolution of medical knowledge, technology, and practice. Practice guidelines are not intended as standards or absolute requirements to replace local institutional policies, and their use cannot guarantee any specific outcome.”
Here’s the big takeaway from the new guidelines: “Quantitative monitoring of neuromuscular blockade is recommended at the adductor pollicis muscle to confirm TOF ratio greater than or equal to 0.9 before extubation, accompanied by the use of Sugammadex or neostigmine for the antagonism of blockade.”
As we review the eight recommendations for the type of monitoring, location of monitoring, and reversal medications keep in mind that recommendations 1-6 are classified as strong recommendations with moderate evidence strength and the seventh and eight recommendations are conditional recommendations with low and very low evidence strength, respectively.
When was the last time that you administered neuromuscular blocking drugs? Perhaps, it was the last time you were in the operating theatre. Did you know that the incidence of residual blockade at the end of surgery or in the PACU may be as high as 64%? This is a big threat to anesthesia patient safety since residual blockade is associated with the following complications:
- Upper airway obstruction
- Reintubation
- Atelectasis
- Pneumonia
- Prolonged PACU stay.
- Decreased patient satisfaction.
How do. you monitor neuromuscular blockade? Historically, qualitative monitors were used, but newer quantitative monitors are available. Quantitative monitoring with peripheral nerve stimulators involves the delivery of four short electrical pulses. The amplitude of the fourth twitch is divided by the amplitude of the first twitch, and this results in the train-of-four ratio. The baseline train-of-four in an unparalyzed patient should be 1.0 since all twitches should have equal amplitude. The TOF ratio decreases with increasing muscle paralysis. Recovery from neuromuscular blockade likely occurs with a TOF ratio greater than or equal to 0.9. Multiple studies have shown that there are significant benefits from using quantitative monitoring of neuromuscular blockade. However, many anesthesia professionals continue to use qualitative monitors leaving patients at risk for residual paralysis. We can look at the literature to help identify factors associated with slow adoption of quantitative monitoring. Check out the 2019 international study in Anesthesia and Analgesia, “Anesthesiologists’ overconfidence in their perceived knowledge of neuromuscular monitoring and its relevance to all aspects of medical practice: an international survey.” I will include this citation in the show notes as well. Here are the factors that were identified in the study:
- Anesthesia professionals’ overconfidence in neuromuscular blockade depth assessment
- Underappreciation of the frequency of residual blockade and the associated complications
- Lack of commercially available quantitative TOF monitors that are easy to use and inexpensive.
Qualitative monitoring for neuromuscular blockade continues to be used. This monitoring involves peripheral nerve stimulation while performing visual or manual/tactile evaluation to complete a subjective assessment of thumb movement for a train-of-four count. Unfortunately, qualitative assessment can mot identify and prevent clinically significant weakness since fade may not be reliably assessed until the TOF ratio is less than 0.4. This means that a TOF ratio between 0.4-0.9 may look and feel the same using qualitative monitoring for neuromuscular blockade. Other qualitative assessments may include sustained head lift or grip strength. Once again, these methods are not sensitive to detect residual blockade since there are many patients with a TOF ratio less than 0.7 who are able to perform a sustained head lift. Another important consideration is that the duration of action of neuromuscular blocking medications may vary depending on the patient so that it is not possible to use time intervals to predict the depth of neuromuscular blockade. This brings us to the first two recommendations based on 11 studies that reported decreased incidences of residual neuromuscular blockade when quantitative monitoring was used compared with qualitative or clinical assessment. Here are the recommendations:
Recommendation 1: When neuromuscular blocking drugs are administered, clinical assessment alone is not recommended to avoid residual neuromuscular blockade.
Recommendation #2: Quantitative monitoring is recommended over qualitative assessment in order to reduce the risk for residual neuromuscular blockade.
Historically, a TOF ratio less than 0.7 was considered the cutoff for residual neuromuscular blockade since vital capacity and inspiratory force had returned to almost normal at that level, but there is evidence that patients continue to experience clinical symptoms of weakness with a train of four ratio less than 0.9. This brings us to the third recommendation which states that a TOF ratio greater than or equal to 0.9 should be confirmed prior to extubation since there is a lower incidence of residual neuromuscular blockade compared to when the TOF ratio was not confirmed to recover to this level.
There are several different types of quantitative TOF monitors available including acceleromyography, electromyography, kinemyography, and mechanomyography. You can click on the link in the article to take you to two supplemental tables for a summary of the last 30 years of data on these different technologies including agreement between the technologies as TOF differences at a given TOF ratio and as time to attain a given TOF ratio. I will include that link in the show notes as well for reference. There are differences between the different types of quantitative monitors, but there is no preferred type recommended in the guidelines.
The location of monitoring is an important consideration since it is important that all muscles recover from the neuromuscular blockade. Studies have revealed that eye muscles are relatively resistant to neuromuscular blocking drugs compared to the adductor pollicis muscle and the recovery time to a TOF ratio greater than or equal to 0.9 at the adductor pollicis muscle is longer compared to the eye muscles. We have now reached the fourth and fifth recommendations which are to use the adductor pollicis muscle for neuromuscular monitoring and to avoid using the eye muscles. There may be time when only the eye muscles are accessible during the case for neuromuscular monitoring due to patient positioning or the surgical procedure. For these cases, it is recommended to change the monitoring location to the adductor pollicis muscle prior to reversal and extubation.
Next up, let’s talk about reversal or antagonism of neuromuscular blockade. Keep in mind that this depends on the depth of the blockade. Check out Table 1 in the article, Depths of Neuromuscular Blockade by Quantitative and Qualitative Measurement. This comes from the 2018 Consensus Statement on Perioperative Use of Neuromuscular Monitoring. From the table, we can see similarities between peripheral nerve stimulator and qualitative assessment and quantitative monitoring for complete, deep, and moderate depth of blockade. However, once the train of four count reaches 4, there are important differences between qualitative and quantitative monitoring respectively:
For shallow blockade, fade is present compared to a TOF ratio less than 0.4.
For Minimal blockade, fade is absent compared to a TOF ratio between 0.4-0.9
For Acceptable Recovery, this cannot be determined compared to a TOF ratio greater than or equal to 0.9.
Now, that we have reviewed depth of blockade, let’s talk about reversal. Remember, aminosteroid neuromuscular blocking medications can be reversed in two ways. First, anticholinesterases inhibit acetylcholinesterase and butyrylcholinesterase which leads to increased presence of acetylcholine at the neuromuscular junction. Neostigmine was evaluated in the practice guidelines since edrophonium is no longer available in the United States. The second option for antagonism is Sugammadex which is a selective relaxant binding agent for reversal of rocuronium and vecuronium. Sugammadex is more effective than neostigmine for antagonism of deep, moderate, and shallow blockade levels. The sixth recommendation from the guidelines is for Sugammadex to be used for antagonism of deep, moderate, and shallow levels of neuromuscular blockade. Are you using Sugammadex in your anesthesia practice? Remember, the FDA-approved doses of Sugammadex for the reversal of rocuronium or vecuronium are:
- 2mg/kg for a TOF count of 2 up to a TOF ratio less than 0.9.
- 4mg/kg for a post-tetanic count of 1 up to a TOF count of 1.
- 16mg/kg for immediate reversal following administration of a single dose of rocuronium of 1.2mg/kg.
There is still an important role for neostigmine for reversal of minimal blockade when the TOF ratio is between 0.4 and 0.9. The seventh recommendation states that Neostigmine is a reasonable alternative to Sugammadex for antagonism of minimal neuromuscular blockade. Keep in mind that with qualitative monitoring, you cannot determine adequate recovery with a TOF ratio greater than or equal to 0.9 and reversal with neostigmine for deeper levels of blockade will vary between patients. According to the guidelines, when Neostigmine is used for antagonism of a block deeper than minimal, it will take more time for recovery to a TOF ratio greater than or equal to 0.9.
There is good news about adverse effects from Sugammadex and neostigmine co-administered with glycopyrrolate. There are over 75 studies cited in the practice guidelines and there appears to be no difference in the incidence of pulmonary complications, anaphylaxis, bradycardia, or tachycardia, postoperative nausea, and postoperative vomiting.
When atracurium and Cisatracurium are used for neuromuscular blockade, there is only one option for reversal, acetylcholinesterase inhibitors. Following reversal with neostigmine, the maximal effect occurs within 10 minutes and efficacy is significantly improved for reversal of minimal blockade compared to deeper block levels. This brings us to our eighth and final recommendation: To avoid residual neuromuscular blockade when qualitative assessment is used, antagonism of a Cisatracurium or atracurium-induced block should not be initiated before there is absence of subjectively assessed fade in the train of four response and at least 10 minutes should elapse from antagonism with neostigmine to extubation. When quantitative monitoring is used, extubation can be done once the train of four ratio is greater than or equal to 0.9.
We made it to the end of the article and through all eight recommendations. Residual neuromuscular blockade is a threat to anesthesia patient safety and these new guidelines can help keep patients safe with quantitative monitoring at the adductor pollicis muscle to confirm a TOF ratio greater than or equal to 0.9 prior to extubation with the use of Sugammadex or neostigmine for reversal. The authors point out that when quantitative monitoring is not available, qualitative monitoring may be used to guide dosages and timing of administration of reversal agents.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
The 2023 APSF Stoelting Conference is happening now, September 6-7th, on “Emerging Medical Technologies – A Patient Safety Perspective on Wearables, Big Data and Remote Care” and you can tune in from anywhere is the world by checking out our livestream on YouTube. So go ahead and subscribe to the Anesthesia Patient Safety YouTube Channel and check out the conference livestream on September 6-7th for the latest on medical technology and anesthesia patient safety.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2023, The Anesthesia Patient Safety Foundation
