Episode #163 Keeping Patients From Opioid-Induced Respiratory Depression
August 15, 2023
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is “Opioid Induced Respiratory Depression— Beyond Sleep Disordered Breathing” by Toby Weingarten.
Here are the citations that we discuss on the show today:
- Weingarten TN, Chong EY, Schroeder DR, Sprung J. Predictors and outcomes following naloxone administration during Phase I anesthesia recovery. J Anesth.2016;30:116–122. PMID: 26449674
- Schumann R, Harvey B, Zahedi F, Bonney I. Minute ventilation assessment in the PACU is useful to predict postoperative respiratory depression following discharge to the floor: A prospective cohort study. J Clin Anesth. 2019;52:93–98. PMID: 30227321
- Khanna AK, Bergese SD, Jungquist CR, et al. Prediction of opioid-induced respiratory depression on inpatient wards using continuous capnography and oximetry: an international prospective, observational trial. Anesth Analg.2020;131:1012–1024. PMID: 32925318
Here is a proposed new approach to postoperative opioid-induced respiratory depression:
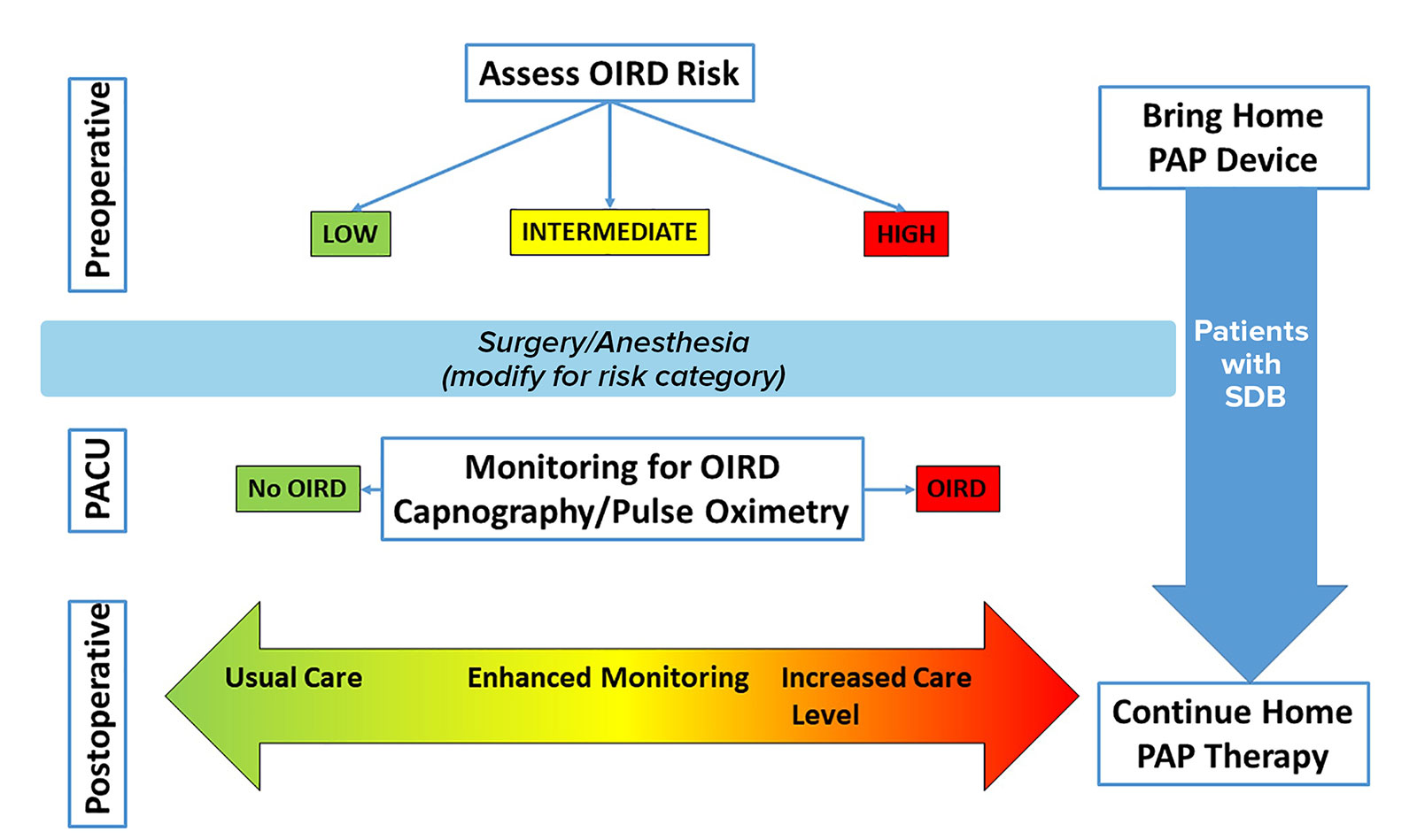
Figure 2: Proposed Clinical Pathway for Patients with Postoperative Opioid-Induced Respiratory Depression.
Clinical decisions on the postoperative level of care are complex and unique for each patient. Preoperatively, patients should have a risk assessment for respiratory depression. The surgical and anesthetic management should be tailored for this risk. During anesthesia recovery, patients’ respiratory status should be monitored for various signs of respiratory depression. Postoperative management decisions regarding level of monitoring and care should be guided by preoperative status, intraoperative status, and the anesthesia recovery course. Home therapies for sleep-disordered breathing should be continued into the postoperative period. PACU indicates postanesthesia care unit; OIRD, opioid induced respiratory depression; SDB, sleep disordered breathing; PAP, positive airway pressure.
Subscribe to our YouTube Channel here: https://www.youtube.com/@AnesthesiaPatientSafety
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2023, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We are continuing to explore the awesome articles from the June 2023 APSF Newsletter. We hope you tuned in last week when we discussed some very important anesthesia patient safety considerations related to opioid medications and we are going to continue the conversation today.
Before we dive into the episode today, we’d like to recognize Preferred Physicians Medical Risk Retention Group, a major corporate supporter of APSF. Preferred Physicians Medical Risk Retention Group has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Preferred Physicians Medical Risk Retention Group – we wouldn’t be able to do all that we do without you!”
Our featured article today is once again “Opioid Induced Respiratory Depression— Beyond Sleep Disordered Breathing” by Toby Weingarten. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue. Then, scroll down until you get to our featured article today. I will include a link in the show notes as well.
Last week, we talked about the APSF’s call to action in 2011 that “no patient should be harmed by opioid-induced respiratory depression in the postoperative period.” We discussed patient characteristics that increase the risk for opioid-induced respiratory depression. High risk patients include the following:
- Patients with obstructive sleep apnea and other sleep breathing disorders
- Older patients
- Male sex
- Congestive heart failure
- Opioid-naivety
- As well as patients with cardiovascular disease, central neurologic disease, and debility
Do you have a protocol for patients who develop postoperative respiratory depression in PACU? Last week, we also reviewed the protocol at the Mayo Clinic to help manage patients in the post-operative care unit who develop respiratory depression. Here’s their protocol.
- First, the patient’s risk for OSA is assessed preoperatively and postoperatively.
- PACU nurses continuously monitor patients for respiratory depression as evidenced by:
- Apnea
- Bradypnea
- Oxyhemoglobin desaturation
- “Pain-sedation” mismatch, this is when a heavily sedated patient complains of severe pain.
- Any patient who has an episode of respiratory depression must then have monitoring for two additional 30-minute periods to evaluate for further episodes of respiratory depression.
- Patients who continue to have episodes of respiratory depression during the additional monitoring period must then have continuous postoperative monitoring with telemetry and may be considered for non-invasive positive pressure ventilation.
The anesthetic plan for patients at high risk for opioid-induced respiratory depression must include consideration for perioperative medications that may further increase the risk for postoperative respiratory depression. These medications include:
- Use of Isoflurane
- Preoperative sustained release oxycodone administration
- Increasing doses of intraoperative opioids
- Preoperative gabapentin administration and continuation of chronic gabapentin administration
Today, we are continuing the discussion and we will be covering Anesthesia Recovery, the Presentation of Opioid-induced Respiratory Depression, and a proposed new approach to this big threat to anesthesia patient safety.
The immediate postoperative period in the PACU may provide information about the future risk of opioid-induced respiratory depression on the postoperative general care wards. Patients who develop respiratory depression in the PACU are at increased risk for postoperative pulmonary complications. Up to one third of patients who screen positive for OSA and experience respiratory depression in the PACU go on to develop postoperative pulmonary complications. The Mayo clinic naloxone studies revealed that respiratory depression in the PACU was associated with a 5-fold increased risk for naloxone administration. Another study by Weingarten and colleagues found that after patients who receive naloxone in the PACU are discharged to the general ward, there is a 3-fold increased risk for postoperative adverse events compared to patients who did not receive naloxone in the PACU. Weingarten tells us that the association between PACU respiratory depression and adverse respiratory events following PACU discharge even after meeting PACU discharge criteria may be due to persistent respiratory depression during anesthesia recovery.
Let’s look at the 2019 study by Schumann and colleagues, “Minute ventilation assessment in the PACU is useful to predict postoperative respiratory depression following discharge to the floor: A prospective cohort study.” In this study, 119 patients were continuously monitored with bioimpedance for minute ventilation after admission to PACU and for 12 hours postop on the general wards. The investigators discovered that patients who experienced low minute ventilation events in the PACU continued to have these events for the next 10 hours on the ward. On the other hand, patients with normal minute ventilation in the PACU continued to have normal minute ventilation on the wards. I will include these citations in the show notes as well.
Next, we are going to review the presentation of opioid-induced respiratory depression and anesthesia professionals must understand the onset timing, signs, and symptoms in order to keep patients safe with appropriate monitoring. How does opioid-induced respiratory depression present? Does this critical event mostly occur overnight following administration of opioids and other sedating medications combined with OSA during sleep? If we go back to the PRODIGY trial that we talked about last week…Remember, this is the 2020 study that evaluated opioid-induced respiratory depression using capnography and oximetry on the general wards. A secondary analysis of this data revealed that there is a complex relationship between opioid-induced respiratory depression, surgery, and time of day. Patients included in this study began to have multiple episodes of postoperative respiratory depression in the late afternoon and early evening between 1600 and 2200 just after arriving on the wards. Then, there were increased events in the early morning hours between 2 and 6AM. Looking at the Mayo Clinic naloxone studies, naloxone administration usually occurred during the afternoon and evening. Keeping patients safe from opioid-induced respiratory depression, likely requires postoperative monitoring that start when patients are admitted to the ward and continues overnight.
It is also important to be aware of the presentation for opioid-induced respiratory depression. In some cases, patients may present with bradypnea and/or hypoxemia, but this is not always the case. Studies have found that patients may have normal respiratory rates and oxygen saturations just prior to severe episodes of opioid-induced respiratory depression. Weingarten provides some possible explanations. It may be that severe events develop all of a sudden so that signs of respiratory depression are not seen during the preceding vital signs check. This explanation is not supported by the literature. Studies have shown that postoperative opioid-induced respiratory depression continues to occur as multiple and repetitive events following PACU discharge. Perhaps, opioid-induced respiratory depression does not present with decreased respiratory rate and oxygen desaturation. From the PRODIGY trial data with continuous capnography and pulse oximetry, almost every episode included apnea or partial apnea with rare bradypnea or oxygen desaturation. Check out Figure 1 in the article for a visual representation. In addition, patients receiving supplemental oxygen experienced periods of apnea without associated oxygen desaturation. It may be that in the setting of a repetitive apnea opioid-induced respiratory depression breathing pattern, when the nurse arrives for a routine assessment, the patient wakes up and resumes a normal breathing pattern so that there is no evidence of the underlying respiratory depression. At the same time, nursing notes may describe the patient as sedated or somnolent and this provides an important clue that the patient may be experiencing respiratory depression. Keeping patients safe may include training nurses to quietly observe breathing patterns of sleeping patients prior to taking additional vital sign measurements that may wake the patient. In addition, it is important to provide education to nursing staff that patients who appear sedated or somnolent are at higher risk for severe respiratory depression and require additional monitoring.
We made it to the end of the article and Weingarten offers a proposed new approach to postoperative opioid-induced respiratory depression. Check out Figure 2 in the article and we are going to review it now. The preoperative phase includes screening for obstructive sleep apnea as well as considering additional characteristics of increasing age and overall disease burden. The PRODIGY score is an easy and convenient screening option that may be included in the electronic health record as well. In addition, patients should be instructed to bring their positive-airway pressure machine from home and continue to use it throughout the perioperative period. During the intraoperative phase, it is important to consider modifications depending on the patient’s risks such as using regional blocks shorter acting agents, and non-sedating analgesics. During the postoperative phase, appropriate monitoring for opioid-induced respiratory depression is critical. Patients who do not experience any episodes and who are at low risk may have usual care on the general ward. Intermediate risk patients may require enhanced monitoring postoperatively. High risk patients who experience respiratory depression in the PACU, likely require increased level of care and monitoring during the postoperative phase to help prevent critical events of opioid-induced respiratory depression. I will include the Proposed Clinical Pathway for Patients with Postoperative Opioid-Induced Respiratory Depression in the show notes as well. This may be something that you can use at your institution to help keep patients safe during anesthesia care.
Before we wrap up for today, we are going to hear from Weingarten again. I also asked him, what’s next for your research. Here’s his response.
[Weingarten] “Our research has suggestive that we as healthcare providers have real difficulty appreciating respiratory depression in actual patients. But we are pretty good at determining the level of sedation in a patient who has on-going respiratory depression. My big question for the future is how to overcome this gap in our patient assessment? Could it be education, new ways of training, or technology? I am not sure but am excited to uncover what’s next.”
[Bechtel] Once again, thank you to Weingarten for contributing for the show today. We cannot wait to learn more about how to better assess patients with respiratory depression going forward to help keep them safe.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
We still have more articles from the June 2023 APSF Newsletter to talk about on this podcast and we hope that you will tune in next week. For more great patient safety content, you can connect with us on Twitter, Instagram, Facebook, and LinkedIn. And don’t forget to subscribe to our YouTube channel to see patient safety videos, conference recaps, podcast episodes and more. Check out the show notes for more information and subscribe today.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2023, The Anesthesia Patient Safety Foundation
