Episode #162 No Patient Should Be Harmed by Opioid-Induced Respiratory Depression
August 8, 2023
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
Our featured article today is “Opioid Induced Respiratory Depression— Beyond Sleep Disordered Breathing” by Toby Weingarten.
The call to action started over ten years ago when the APSF stated that “no patient should be harmed by opioid-induced respiratory depression in the postoperative period.” Check out the Fall 2011 APSF Newsletter article by Weinger and Lee, “No Patient Shall be Harmed by Opioid-Induced Respiratory Depression.”
Table 1: PRODIGY Scoring System for Assessing Risk for OIRD Among Patients Hospitalized on General Care Wards Receiving Opioids
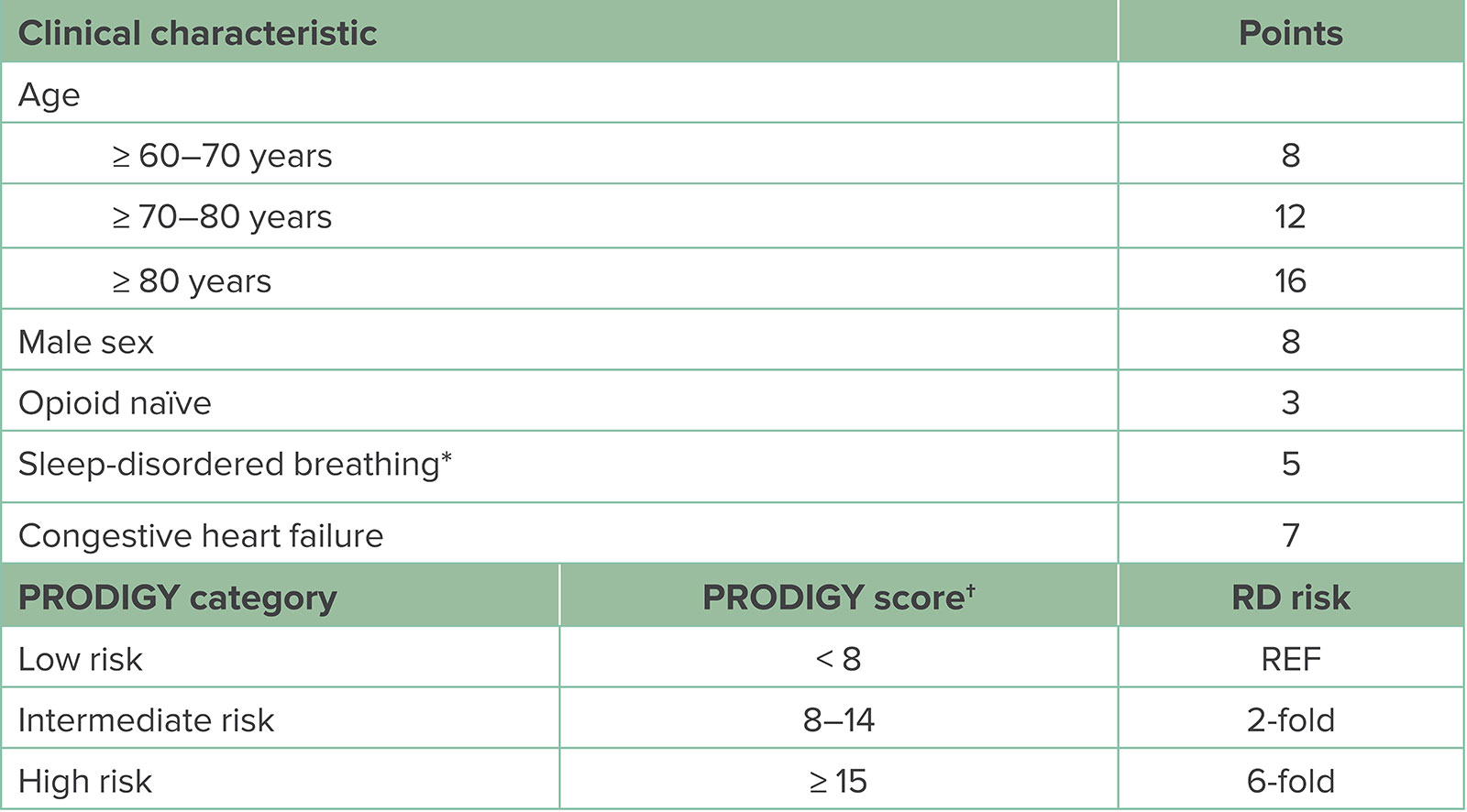
Abbreviations: PRODIGY, PRediction of Opioid-induced respiratory Depression in patients monitored by capnoGraphY; RD, respiratory depression; REF, reference range.
*Sleep-disordered breathing can be determined from either patient history or positive screen for sleep apnea.
†To calculate the PRODIGY risk score, summate the assigned points per positive clinical characteristic. Patients are assigned low-, intermediate-, or high-risk category based on the number of points. Compared to low-risk scored patients, intermediate-risk patients have a 2-fold increase and high-risk patients a 6-fold increased risk for experiencing respiratory depressive episodes on the general care ward. (Adapted from Khanna et al.7)
Here are the citations to the studies that we talked about on the show today:
- Deljou A, Hedrick SJ, Portner ER, et al. Pattern of perioperative gabapentinoid use and risk for postoperative naloxone administration.Br J Anaesth. 2018;120:798–806. PMID: 29576120
- Weingarten TN, Herasevich V, McGlinch MC, et al. Predictors of delayed postoperative respiratory depression assessed from naloxone administration.Anesth Analg. 2015;121:422–429. PMID: 25993390
- Khanna AK, Bergese SD, Jungquist CR, et al. Prediction of opioid-induced respiratory depression on inpatient wards using continuous capnography and oximetry: an international prospective, observational trial. Anesth Analg.2020;131:1012–1024. PMID: 32925318
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2023, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We are continuing to explore the awesome articles from the June 2023 APSF Newsletter. When was the last time you administered an opioid or ordered opioids for postoperative pain control? For many anesthesia professionals, this is something that we do on a routine basis. There are also some very important anesthesia patient safety considerations related to opioid medications that we are going to discuss today.
Before we dive into the episode today, we’d like to recognize Medtronic, a major corporate supporter of APSF. Medtronic has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, Medtronic – we wouldn’t be able to do all that we do without you!”
Our featured article today is “Opioid Induced Respiratory Depression— Beyond Sleep Disordered Breathing” by Toby Weingarten. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the current issue. Then, scroll down until you get to our featured article today. I will include a link in the show notes as well.
Before, we get into the article, we are going to hear from the author. Here he is now.
[Weingarten] “Hi, my name is Toby Weingarten, and I am a professor of Anesthesiology at the Mayo Clinic in Rochester MN.”
[Bechtel] To kick off the show today, I asked Weingarten why he is so passionate about this topic. Let’s take a listen to what he had to say.
[Weingarten] “I have been researching postoperative respiratory depression for many years and our team has found surprising but consistent patterns of how and when respiratory depression develops. I strongly believe that by sharing our observations the anesthesia community can help patients have a safer perioperative course.”
[Bechtel] Thank you so much to Weingarten for contributing to the show today and for sharing what you have learned from your research. Before we get into the article, we are going to head back in time and into our archives.
The call to action started over ten years ago when the APSF stated that “no patient should be harmed by opioid-induced respiratory depression in the postoperative period.” Check out the Fall 2011 APSF Newsletter article by Weinger and Lee, “No Patient Shall be Harmed by Opioid-Induced Respiratory Depression.” I will include a link to this article from our archives in the show notes as well. This article summarizes the proceedings from the APSF multidisciplinary conference, “Essential Monitoring Strategies to Detect Clinically Significant Drug-Induced Respiratory Depression in the Postoperative Period” held in June 2011. At this conference, participants were asked the following questions.
- Should electronic monitoring be utilized to facilitate detection of drug-induced postoperative respiratory depression?
- If “Yes” to electronic monitoring, who should be monitored (inclusively or selectively) and what monitors/technology should be utilized?
The article reviews all the speakers and sessions from the conference, but we are going to skip ahead to the conclusion. The conference attendees reached the following consensus:
- Continual electronic monitoring should be used for inpatients receiving postoperative opioids. Pulse oximetry is likely the most reliable and practical when patients are not receiving supplemental oxygen. For patients receiving supplemental oxygen, capnography may be necessary to detect hypoventilation.
- Improved education is needed for all care providers regarding the risks related to postoperative opioid administration and for accurate assessment of sedation levels to help prevent opioid-induced respiratory depression.
- If resources are limited, a staged postoperative monitoring implementation may be necessary starting with the highest risk patients first, but with the goal for universal postoperative monitoring for patients receiving opioids. Keep in mind that risk stratification alone will not prevent postoperative opioid-induced respiratory depression.
Now, that we have seen where we were in 2011, let’s turn our attention back to our featured 2023 article.
Since then, research studies have established the link between obstructive sleep apnea, or OSA, and adverse events following opioid use in the postoperative period. The response from the American Society of Anesthesiologists included updated practice guidelines in 2014 for perioperative management for patients with OSA recommending screening for OSA, continuing OSA therapies including CPAP during the postoperative period, and adjusting the anesthetic management and postoperative monitoring if needed for patients with OSA. However, this remains an ongoing problem and the rates of severe postoperative opioid-related respiratory depression have remained constant. There is some good news though since recent studies have provided further knowledge about identifying patients at highest risk for opioid-induced respiratory depression beyond screening for OSA and about when and how this happens so that we can implement improved postoperative monitoring strategies going forward.
Next, let’s take a closer look at the characteristics of patients who are at high risk for opioid induced respiratory depression. We know that there is an association between opioid-induced respiratory depression and OSA. Research studies at the Mayo Clinic evaluated administration of naloxone on postoperative wards as a way to study severe events related to opioid-induced respiratory depression. The studies revealed that patients with a history of OSA or patients who screened positive for OSA had two times the risk for developing severe postoperative respiratory depression following opioid administration.
We also need to talk about the PRODIGY trial, which stands for the Prediction of Opioid-induced respiratory depression in patients monitored by capnography trial. This study used bedside capnography and pulse oximetry on the general ward to evaluate episodes of opioid-induced respiratory depression. Check out Figure 1 in the article which shows a capnography and pulse oximetry reading from the PRODIGY trial and demonstrates the typical breathing pattern seen with opioid-induced respiratory depression. This patient is experiences episodes of apnea and partial apnea with intermittent normal breathing patterns. There are also periods of hypoxemia during the episodes of apnea with resolution during the normal breathing patterns. The PRODIGY researchers created the PRODIGY scoring system which you can find in the article as Table 1, and I will include it in the show notes as well. This scoring system may be used for assessing risk for opioid induced respiratory depression for patients hospitalized on the general ward.
Let’s review this scoring system now. It includes clinical characteristics and an assigned point score.
First up is age with the following:
- Greater than or equal to 60-70 years old for 8 points
- Greater than or equal to 70-80 years for 12 points
- Greater than or equal to 80 years for 16 points
- Second is Male Sex for 8 points.
- Then, Opioid naïve for 3 points.
- Sleep-disordered breathing is worth 5 points.
- Congestive heart failure is 7 points.
Add up the points to determine the total score.
- A score less than 8 is low risk and serves as the reference range for the respiratory depression risk.
- A score between 8-14 is Intermediate Risk with a 2-fold increased risk for respiratory depression.
- A score that is greater than or equal to 15 is high risk with a 6-fold increased risk for respiratory depression following opioid administration.
The PRODIGY trial helped to identify patients at high risk for opioid induced respiratory depression. Be on the lookout for patients with OSA and other sleep breathing disorders, older patients, male sex, congestive heart failure, and opioid naivety. Weingarten points out that a weakness of the PRODIGY trial is that many of the 46 factors that were evaluated in the study were specific diagnoses and some were just too rare to adequately examine, for example amyotrophic lateral sclerosis. Going back to the Mayo Clinic studies, these studies looked at organ system disease and the associated risk. The studies revealed that cardiovascular disease, OSA, and debility more than doubled the risk for opioid induced respiratory depression. The presence of central neurologic disease was found to quadruple the risk. Anesthesia professionals should be aware that patients with OSA, increasing age, disease burden, and debility are all risk factors in order to keep patients receiving opioids safe following anesthesia care. I will include these citations in the show notes as well.
Now, let’s turn our attention to the perioperative course and its impact on respiratory depression. Patients undergoing longer and more invasive procedures are at higher risk for respiratory failure. On the other hand, when regional anesthesia is used, this may help to decrease the risk. What about the impact of different anesthetic drugs? These are important considerations as we try to keep patients safe from opioid-induced respiratory depression. Let’s take a look at the protocol used at the Mayo Clinic to manage patients in the post-operative care unit who develop respiratory depression.
- First, the patient’s risk for OSA is assessed preoperatively and postoperatively.
- PACU nurses continuously monitor patients for respiratory depression as evidenced by:
- Apnea
- Bradypnea
- Oxyhemoglobin desaturation
- “Pain-sedation” mismatch, this is when a heavily sedated patient complains of severe pain.
- Any patient who has an episode of respiratory depression must then have monitoring for two additional 30-minute periods to evaluate for further episodes of respiratory depression.
- Patients who continue to have episodes of respiratory depression during the additional monitoring period must then have continuous postoperative monitoring with telemetry and may be considered for non-invasive positive pressure ventilation.
Pre-op and intraoperative medications may increase the risk for postoperative respiratory depression as well. Increased risk may occur in the following situations:
- Use of Isoflurane
- Preoperative sustained release oxycodone administration
- Increasing doses of intraoperative opioids
- Preoperative gabapentin administration
Using desflurane instead of isoflurane and decreasing routine midazolam use were associated with a 30% decrease in episodes of PACU respiratory depression at one Mayo Clinic site.
In the past, many enhanced recovery after surgery protocol included administration of gabapentin and pregabalin to help improve postoperative pain and decrease opioid requirements. Let’s look closer at the literature in this area. Studies have shown that gabapentin and pregabalin continue to increase the risk for respiratory depression even after discharge from the PACU. The 2018 study by Deljou and colleagues, “Pattern of perioperative gabapentinoid use and risk for postoperative naloxone administration” revealed that patients taking gabapentin at home prior to surgery with continued use postoperatively had a 6-fold increased risk for naloxone administration. Another study looked at the Premier Healthcare Database and found that preoperative gabapentin and pregabalin administration as part of an ERAS protocol was associated with an increased risk for postoperative pulmonary complications after colorectal, gynecological, and joint replacement surgeries. In addition, the Federal Drug Administration or FDA has issued a black box warning that administration of gabapentin or pregabalin with other sedative medications increases the risk for severe respiratory complications. We must also consider that both of these medications only provide weak analgesia benefits when used during surgery combined with the potential for opioid-induced respiratory depression. The risks likely outweigh benefits for using gabapentin and pregabalin as part of ERAS protocols and it may be necessary to modify these protocols in order to keep patients safe.
There is still so much that we need to talk about including Anesthesia Recovery, the Presentation of Opioid-induced Respiratory Depression, and a proposed new approach to this big threat to anesthesia patient safety. We hope that you tune in next week for the exciting Part 2 episode. Plus, we are going to hear from Weingarten again.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
While waiting for the next Anesthesia Patient Safety Podcast to drop, we hope that you will head over to APSF.org and check out all of the patient safety resources. Head over to APSF.org and click on the Patient Safety Resources heading. There are so many great resources including the COVID Perioperative Resource Center, the Anesthesia Patient Safety Podcast, the APSF Video library, News and Updates, In the Literature, APSF Technology Education Initiative, the Emergency Manuals Implementation Collaborative, the Perioperative Multi-Center Handoff Collaborative, Look-Alike Drug Vials, Drug-Drug Interactions, Innovative Reports and Ideas, International Resources and Helpful Link. What are you waiting for, go check it out!
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2023, The Anesthesia Patient Safety Foundation
