Episode #134 Keeping Patients Safe During Monitored Anesthesia Care for ERCP
January 24, 2023
Welcome to the next installment of the Anesthesia Patient Safety podcast hosted by Alli Bechtel. This podcast will be an exciting journey towards improved anesthesia patient safety.
We are returning to the October 2022 APSF Newsletter for our featured article today, “Pro-Con Debate: Monitored Anesthesia Care Versus General Endotracheal Anesthesia for Endoscopic Retrograde Cholangiopancreatography” by Luke Janik, Samantha Stamper, Jeffrey Vender, and Christopher Troianos.
https://journals.lww.com/anesthesia-analgesia/pages/podcastepisodes.aspx?podcastid=3
Today, we are focusing on the Pre-side of the debate in favor of MAC for ERCP with special guest, Samantha Stamper who contributed audio clips to the show today.
Here are the highlights from the PRO-side including arguments in favor of MAC for ERCP.
- No significant difference in overall serious adverse events when comparing MAC when compared with GEA in healthy nonobese patients.
- Avoidance of the potential problems associated with GEA including intubation-related injury, hemodynamic instability, and medication side effects.
- Improved gastrointestinal suite efficiency metrics and shorter patient recovery time.
- Low conversion rate from MAC to GEA at less than 4%.
- Reliable detection of airway obstruction using end-tidal CO2 monitoring and astute clinical observation, and rapid improvement with basic airway maneuvers.
Check out Table 2 from the article.
Table 2: Advantages and Disadvantages of Each Anesthetic Plan of Care.
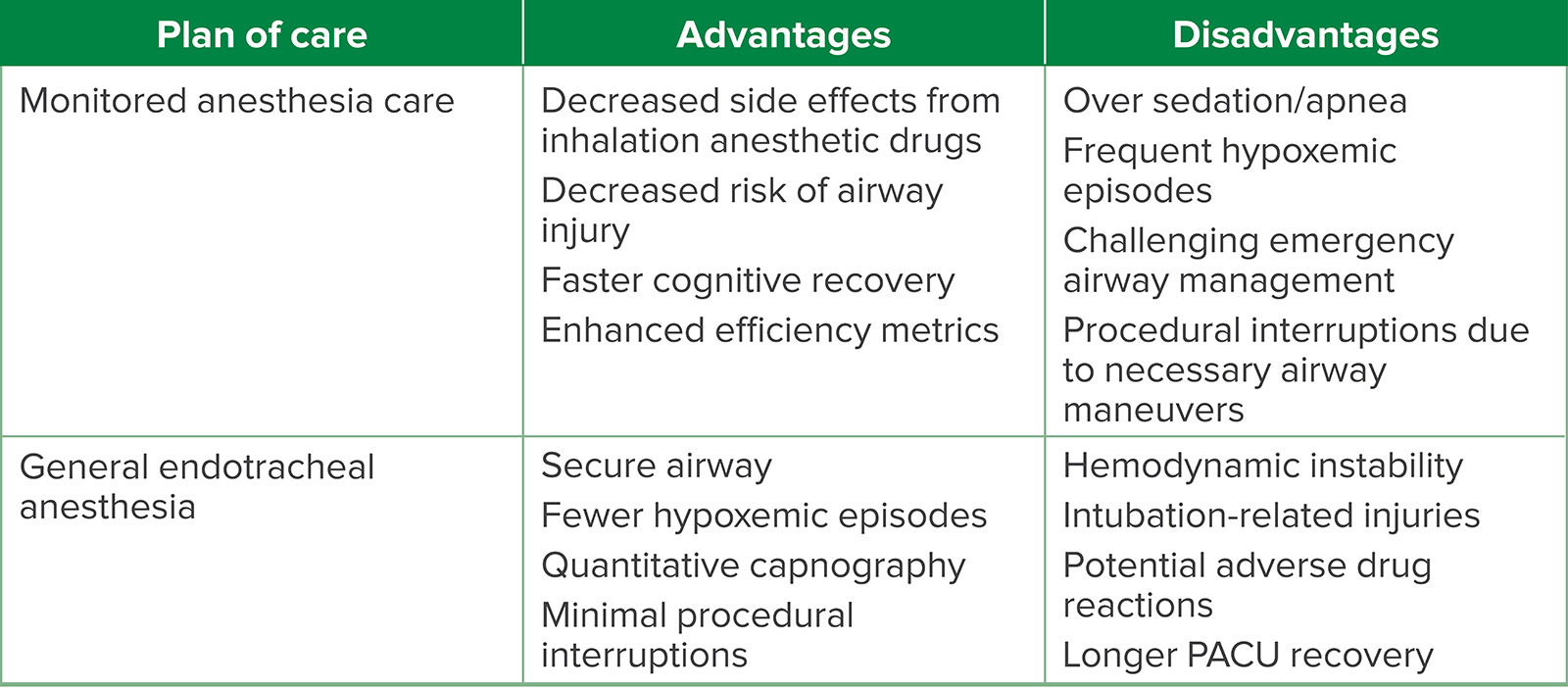
Abbreviation: PACU, postanesthesia care unit.
Be sure to check out the APSF website at https://www.apsf.org/
Make sure that you subscribe to our newsletter at https://www.apsf.org/subscribe/
Follow us on Twitter @APSForg
Questions or Comments? Email me at [email protected].
Thank you to our individual supports https://www.apsf.org/product/donation-individual/
Be a part of our first crowdfunding campaign https://www.apsf.org/product/crowdfunding-donation/
Thank you to our corporate supporters https://www.apsf.org/donate/corporate-and-community-donors/
Additional sound effects from: Zapsplat.
© 2023, The Anesthesia Patient Safety Foundation
Hello and welcome back to the Anesthesia Patient Safety Podcast. My name is Alli Bechtel, and I am your host. Thank you for joining us for another show. We have a very special show today. It is a Pro-Con Debate right here on the podcast.
Before we dive into the episode today, we’d like to recognize ICU Medical, a major corporate supporter of APSF. ICU Medical has generously provided unrestricted support to further our vision that “no one shall be harmed by anesthesia care”. Thank you, ICU Medical – we wouldn’t be able to do all that we do without you!”
We are returning to the October 2022 APSF Newsletter for our featured article today, “Pro-Con Debate: Monitored Anesthesia Care Versus General Endotracheal Anesthesia for Endoscopic Retrograde Cholangiopancreatography” by Luke Janik, Samantha Stamper, Jeffrey Vender, and Christopher Troianos. To follow along with us, head over to APSF.org and click on the Newsletter heading. First one down is the Current Issue, October 2022 and then scroll down until you get to our featured article today. I will include a link in the show notes as well. This article is a reprint from Anesthesia and Analgesia from June 2022 with permission from International Anesthesia Research Society. We are very excited to talk about this article on the show today. This article was also featured on the Article of the Month June 2022 Podcast by Anesthesia and Analgesia Editorial Board with interviewer Richard Prielipp and guests Luke Janik and Samantha Stamper. I will include a link to this podcast episode in the show notes and we hope that you will check it out.
Let’s get into the article. We are discussing anesthesia care for endoscopic retrograde cholangiopancreatography. You may have been involved in providing anesthesia care for this procedure since there are over 500,000 ERCP procedures performed each year in the United States. It involves fluoroscopy and endoscopy to evaluate the liver, gallbladder, bile ducts, and pancreas for diagnostic and therapeutic interventions. Some of the interventions include biliary sphincterotomy, gallstone extraction or fragmentation, biliary and pancreatic duct stenting, and pancreatic pseudocyst drainage. These therapeutic interventions have replaced prior open and laparoscopic surgical procedures.
There are some important considerations for keeping patients safe during this procedure:
- There is a shared airway.
- Positioning may be prone or semi prone on a special procedural table.
- Varied procedure times from less than one hour to several hours long.
Anesthesia techniques for this procedure are varied as well and may include monitored anesthesia care or general endotracheal anesthesia. Additional considerations include patient risk factors and co-morbidities, practitioner skills and experience, procedural needs, and lack of data to define a clear standard of care. What we do know is that a closed claims report from the American Society of Anesthesiologists revealed that adverse events in nonoperating room anesthesia sites leads to a higher incidence of severe complications including death and permanent brain damage when compared to similar events in the operating room. In NORA locations, GI procedures are at the top of the list for adverse events. Anesthesia professionals must remain vigilant especially since there is a high demand for anesthesia care during GI procedures. What was your anesthetic plan the last time you were in the GI suite for an ERCP procedure? Did you debate between MAC or general endotracheal anesthesia? We are going to work through that debate now, so stay tuned.
We are going to get started with the Pro side of this debate. So, to kick off the show, let’s meet one of the authors.
[Samantha Stamper] “Hi, my name is Samantha Stamper and I’m an anesthesiologist at the Cleveland Clinic in Cleveland, Ohio and the co-author of “The Pro Con Debate Monitored Anesthesia Care Versus General Endotracheal Anesthesia for Endoscopic Retrograde Cholangiopancreatography.”
[Bechtel] “I asked Stamper what go her interested in this topic. Let’s take a listen to what she had to say.”
[Stamper] “I was interested in this topic because the amount of time anesthesiologists are spending in non-operating room settings is increasing and will only continue to. I think it’s important to realize that anesthesia is not one size fits all, and each patient requires an individualized plan that is dependent upon many different factors. I really enjoyed getting to participate in this Pro-Con piece. It was initially challenging to be focused on only one side at the debate when the decision for the type of anesthetic you choose varies greatly depending upon the circumstance.
When reading the final piece, it is clear that each side provides supportive data and considerations for patient safety to assist anesthesiologists in determining the most appropriate anesthetic choice for their.”
What a great way to start the show. Here are the highlights from the PRO-side including arguments in favor of MAC for ERCP.
- No significant difference in overall serious adverse events when comparing MAC when compared with GEA in healthy nonobese patients.
- Avoidance of the potential problems associated with GEA including intubation-related injury, hemodynamic instability, and medication side effects.
- Improved gastrointestinal suite efficiency metrics and shorter patient recovery time.
- Low conversion rate from MAC to GEA at less than 4%.
- Reliable detection of airway obstruction using end-tidal CO2 monitoring and astute clinical observation, and rapid improvement with basic airway maneuvers.
In support of MAC for ERCP procedures, you may consider a Mac-first approach. Keep in mind that many of the patients undergoing ERCP procedures are older and may have many significant comorbidities. Utilizing MAC for ERCP may be a superior for healthier patients with normal or near-normal BMI. Another important consideration is making sure to communicate with the endoscopist before and during the procedure. Before the procedure, it is important to determine the indication for the procedure and anticipated case duration to help develop an appropriate and safe anesthetic plan. The authors provide some examples to help differentiate:
- MAC may be the best choice for a straightforward biliary stent removal
- GA with an endotracheal tube may be better for drainage of a complex, septated pancreatic pseudocyst with necrotic walls.
This is a good time to review the advantages and disadvantages of providing MAC for ERCP. Check out Table 2 in the article which highlights the advantages and disadvantages of each anesthetic plan of care. We will review it now and I will include it in the show notes as well.
The advantages of MAC include the following:
- Decreased side effects from inhalation anesthetic drugs
- Decreased risk of airway injury
- Faster cognitive recovery
- Enhanced efficiency metrics
Now for the disadvantages. Here we go.
- Over-sedation or apnea
- Frequent hypoxemic episodes
- Challenging emergency airway management
- Procedural interruptions due to necessary airway maneuvers
There are so many important considerations for keeping patients safe in the GI suite. Some of these facility factors include proximity to the main operating rooms, availability of rescue equipment, adequate post-anesthesia care unit, availability of additional help, and the physical footprint of the anesthesia workspace (which may be very limited from the presence of large pieces of specialized equipment in the room). We have talked about how important communication is in NORA sites and this is definitely true in the GI suite. It is important to have a conversation with the proceduralist about positioning for the ERCP. If the patient will be prone or semi prone, you will need to consider access to the airway and the impact on venous return and cardiovascular stability. The benefits of these positions include maintenance of pulmonary blood flow and ventilation distribution in the lungs especially in non-intubated patients while increasing functional residual capacity and arterial PO2. Plus, the endoscope may act as a stent to help prevent airway collapse.
Are you comfortable proceeding with a MAC anesthetic for a planned prone procedure? A big concern is urgent or emergent airway access and being able to intubate a prone patient. The authors reveal a potential method with the endoscopist performing a gastroscope-facilitated endotracheal intubation with a smaller endoscope placed into the trachea with a pre-loaded endotracheal tube advanced over the scope with the help of an anesthesia professional. There is an “ultraslim” gastroscope with an outer diameter of 5.4mm that an adult endotracheal tube can be placed over similar to a bronchoscope. The good news is that conversion from MAC to general with an endotracheal tube does not occur very often. Let’s take a look at the 2021 review of 3400 patients undergoing ERCP with 46% undergoing general endotracheal anesthesia and 54% with MAC. The conversion rate was only 2.3% between MAC to general. In this study, the authors describe the gastroscope-facilitated tracheal intubation method in 16 patients that was required due to retained food in the stomach and/or hypoxia. The gastroscope may then be used to suction any aspirated material from the trachea and bronchi if needed. In the Barakat study, all of the gastroscope-facilitated intubated patients were successful extubated with no radiographic evidence of aspiration pneumonia.
With appropriate training and anesthesia supervision, the gastroscope-facilitate intubation method may be used to improve patient safety for patients undergoing ERCP in the prone or semi prone position under MAC. An anesthesia professional should be available to perform the procedure or supervision to ensure safe placement of the endotracheal tube. It is also important to quickly switch to the ultraslim gastroscope with a loaded endotracheal tube for the urgent intubation procedure.
It is important to consider the risk factors for sedation-related adverse events. MAC for ERCP is likely to be a safe option for low-risk patients. Check out Table 3 in the article for a list that we are going to review now. Get your pencils ready.
- Obstructive sleep apnea
- Body Mass Index >35
- Male Sex
- ASA Physical Status > III
- Emergent Procedure
- Mallampati IV or Difficult airway
- Severe gastroesophageal reflux disease
- Esophageal/gastric mass
Now, let’s take a look at the literature. There was a large, population-based study at multiple endoscopy centers in the United States revealed no significant difference in serious adverse events during ERCP performed with MAC compared to general. Looking a little closer, the authors revealed that ASA physical status IV patients had a significantly higher risk of adverse events with MAC. Another study evaluated MAC compared to general when the decision was left up to the anesthesia professional with 393 patients undergoing MAC and 45 patients having a general anesthetic for their ERCP. The conversion rate of MAC to GA was 3.7% with a quarter of these patients being ASA physical status IV patients. In addition, there were no significant differences in adverse event rates between MAC and general. Thus, it appears that MAC may be appropriate and safe for ERCP in healthier, nonobese patients after careful evaluation by the anesthesia professional.
We still have so much more to talk about when it comes to performing MAC for ERCP including clinical monitoring, options to provide supplemental oxygen, and the anesthetic plan with a focus on premedication, sedation, and topical anesthetics. We hope that you will tune in next week when we continue the conversation. Before we wrap up for today, we are going to hear from Stamper again. I also got a chance to ask Stamper what she hopes to see going forward. Here is her vision.
[Stamper] “The choice of monitored anesthesia care versus general endotracheal anesthesia for E R C P is the topic that will continue to evoke a lot of discussion amongst anesthesiologists as we see increases in the utilization of anesthesia in non-operating room settings, we will be faced with this decision more often since neither side is supported by large, randomized control trials. It would be nice to see this type of data in the future to aid in our decision-making process.”
[Bechtel] Thank you so much to Stamper for contributing to the show today. Please let us know what side of the debate you are on…MAC or General endotracheal anesthesia for ERCP by tagging us on twitter @APSForg using the hashtag, #APSFpodcast.
If you have any questions or comments from today’s show, please email us at [email protected]. Please keep in mind that the information in this show is provided for informational purposes only and does not constitute medical or legal advice. We hope that you will visit APSF.org for detailed information and check out the show notes for links to all the topics we discussed today.
We hope that you have been enjoying listening to this podcast. Don’t forget to subscribe to the podcast through iTunes or your favorite podcast app and we would love it if you could share this podcast with all of your colleagues, friends, and family and anyone you know who is interested in anesthesia patient safety and don’t forget to leave us a review.
Until next time, stay vigilant so that no one shall be harmed by anesthesia care.
© 2023, The Anesthesia Patient Safety Foundation
