Drew’s Movement
| The following article is provided by the Society of Airway Management (SAM) located online at https://samhq.com/ |
 Drew Hughes’ death inspired a movement. Drew died when his life sustaining breathing tube was unintentionally removed, starving his brain of critical oxygen. Drew’s patient safety event, known as unplanned extubation, is a common cause of preventable death. More than 33,000 patients, in US Intensive Care Units alone, die from this preventable complication of the procedure that is supposed to keep them alive. Inspired by the story of Drew’s tragic death, a coalition was formed, involving eleven major professional medical societies, as well as several patient safety and quality improvement organizations, all with the common goal of increasing awareness and prevention efforts to eliminate these preventable deaths from unplanned extubation.
Drew Hughes’ death inspired a movement. Drew died when his life sustaining breathing tube was unintentionally removed, starving his brain of critical oxygen. Drew’s patient safety event, known as unplanned extubation, is a common cause of preventable death. More than 33,000 patients, in US Intensive Care Units alone, die from this preventable complication of the procedure that is supposed to keep them alive. Inspired by the story of Drew’s tragic death, a coalition was formed, involving eleven major professional medical societies, as well as several patient safety and quality improvement organizations, all with the common goal of increasing awareness and prevention efforts to eliminate these preventable deaths from unplanned extubation.
Drew’s Story
He was young. He was intelligent. He was loved by all. He had a very promising life in front of him. Yet, he died. Needlessly. A preventable death, not from his head injury, but from the complications of the medical treatment that was supposed to sustain his life.
On the evening of June 28, 2013, Drew was skateboarding with his friends, as he did most summer evenings. But this evening, Drew fell, hitting his head. He was taken to the hospital by ambulance. When he arrived, he was awake and alert. He looked fine. But the doctor found a small abnormality on CT Scan. So, for Drew’s safety, the decision was made to transfer him to the level I trauma center. A breathing tube was placed in the ED for his safety during the long transport to the trauma center. However, in the ambulance, Drew’s tube was accidentally removed (extubated). Although the crew replaced the tube, they placed it in his esophagus, and they did not recognize its malposition. His condition quickly worsened. His oxygen levels fell. His heart rate slowed. So, the ambulance diverted to the nearest hospital. But it was too late. Drew had already suffered anoxic brain injury. And he died. He died a preventable death from the complications of airway management.
Unplanned extubation is very common.
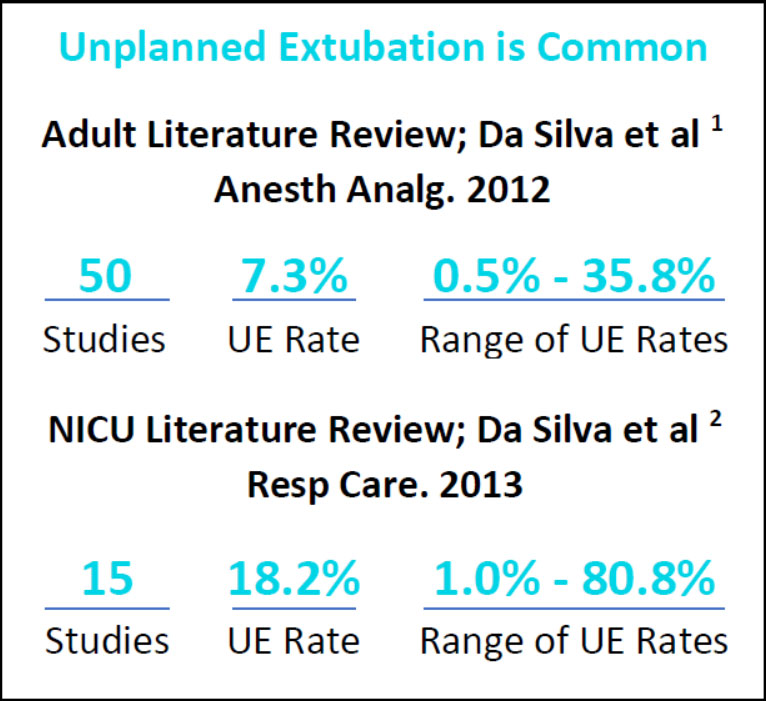 Drew’s death is tragic. But it is not an isolated event. The unintended removal of a patient’s life sustaining breathing tube, unplanned extubation (UE), occurs in over 200,000 patients yearly in the US and results in greater than 50,000 lives lost.
Drew’s death is tragic. But it is not an isolated event. The unintended removal of a patient’s life sustaining breathing tube, unplanned extubation (UE), occurs in over 200,000 patients yearly in the US and results in greater than 50,000 lives lost.
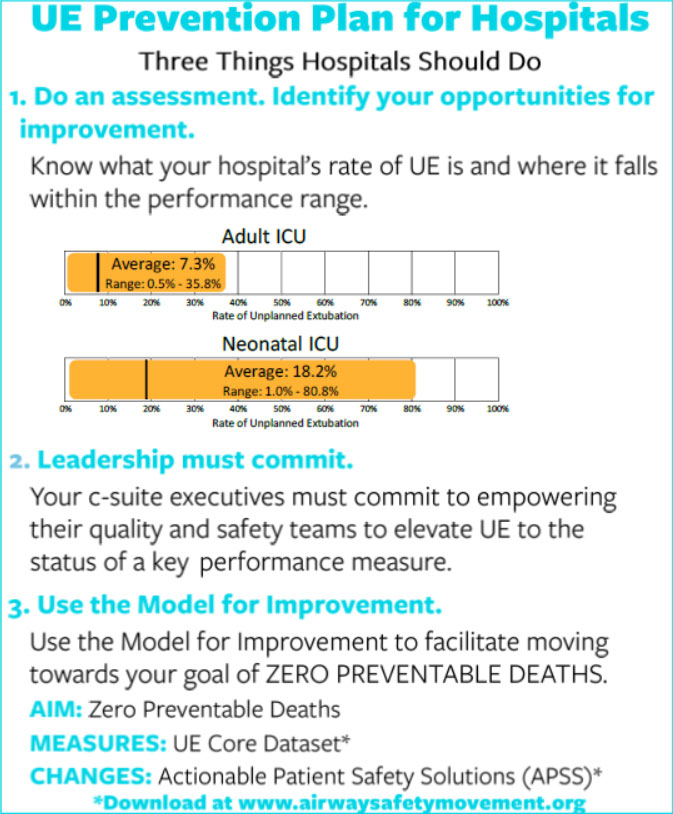
Lucas da Silva’s comprehensive review of fifty articles in the literature involving more 60,000 patients revealed that 7.3% of intubated adult ICU patients experience an unplanned extubation. His comprehensive review of fifteen articles in the neonatal literature revealed 18.2% of intubated neonatal ICU patients experience an unplanned extubation. However, more important than the average is the range of unplanned extubation amongst study institutions. In adults the range is 0.5% – 35.8%. In neonates, the range is 1.0% to 80.8%. This indicates that there is a very large variance in hospitals’ ability to prevent unplanned extubation. It also shows that there is a very large opportunity for improvement.
Does your hospital track unplanned extubation?
Do you know what the rate of UE is in your hospital?
Not knowing does not mean it does not occur.
And not knowing is NOT acceptable, when the outcome is preventable death.
Unplanned Extubation is not only common, it is also costly.
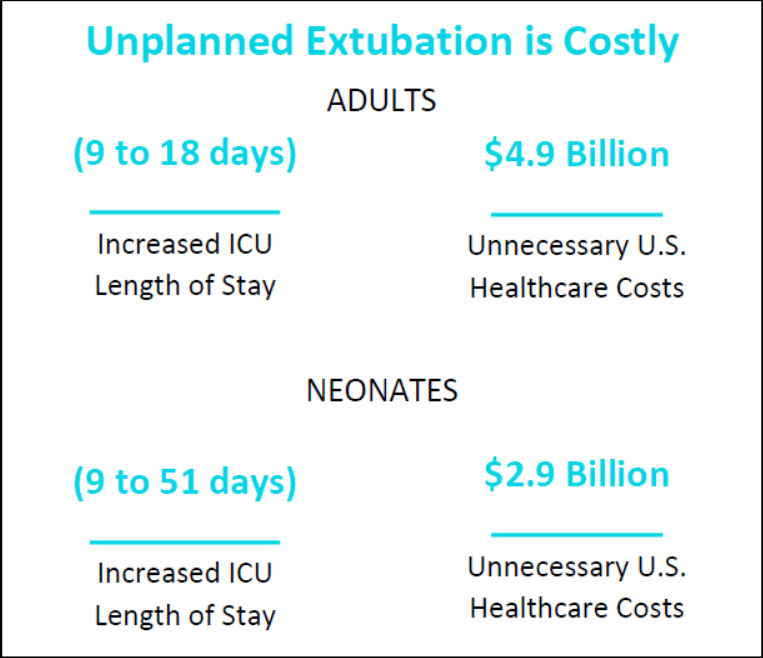 In adults, unplanned extubation increases the average length of stay from 9 to 18 days. This increased length of stay contributes to the average cost of an adult unplanned extubation, which is $40,000. The 121,000 incidents of UE result in wasted healthcare costs of $4.9 Billion.
In adults, unplanned extubation increases the average length of stay from 9 to 18 days. This increased length of stay contributes to the average cost of an adult unplanned extubation, which is $40,000. The 121,000 incidents of UE result in wasted healthcare costs of $4.9 Billion.
In neonates, unplanned extubation increases the average length of stay from 9 to 51 days. This increased length of stay contributes to the average cost of a neonatal unplanned extubation, which is $36,000. The 80,000 incidents of UE result in wasted healthcare costs of $2.9 Billion.
More important than the dollar cost of UE is the loss of life. There are 33,000 deaths yearly associated with UE in adults. The literature does not define relative mortality rates in NICU patients.
However, one life lost from a preventable complication like UE is too many.
Although the literature clearly shows that unplanned extubation is common and costly, the gravity of this problem, at least in the adult world, is uncommonly recognized. Unfortunately, unplanned extubation is thought of simply as a “cost of doing business”. Most institutions do not track unplanned extubation. It is not a key performance measure. And most major electronic health records do not even include the main data field for differentiating when an extubation is planned versus unplanned. In the neonatal world, however, unplanned extubation is well recognized and there are widespread efforts to minimize the risk of unplanned extubation.
The Movement to Increase Awareness and Prevention of Unplanned Extubation
Drew’s story has inspired a movement to increase awareness and prevention of this tragic complication of airway management. A coalition of multispecialty professional medical societies, patient safety and quality improvement organizations led by the Society for Airway Management and the Patient Safety Movement Foundation, has launched a national campaign to reduce the incidence of preventable death from unplanned extubation through increasing awareness, a toolbox of quality improvement best practices for hospitals and support of research and innovation.
| Coalition for Unplanned Extubation Awareness & Prevention |
The Unplanned Extubation Awareness and Prevention Initiative involves efforts to increase awareness of the problem and to provide tools that hospitals can use to take inventory and then initiate programs to work toward zero preventable deaths and harm from unplanned extubation.
Because unplanned extubation is currently not a CMS mandatory key performance measure, many hospitals do not track it as a metric. However, unplanned extubation is on the radar of CMS and likely will become a key performance measure in the future. Therefore, it is important to begin quality improvement efforts now, before it becomes a potential drain on hospitals’ finances.
The coalition has developed the roadmap and the tools necessary to decrease the incidence of preventable harm and death from UE.
There are three things every hospital should do to move toward zero preventable harm:
- Take inventory. Do an assessment. Determine what your hospital’s rate of unplanned extubation is. Once you know what your rate of UE is, then determine where it falls on the performance range. The farther to the right that your rate falls on the performance range, the larger the opportunity for improvement. Know where you fall. Set goals for improvement.
- You must obtain the support of your C-Suite executives. They must commit to empowering your quality and safety teams to elevate UE to the status of a key performance measure and provide the resources necessary for this critical quality improvement measure.
- Develop a Quality Improvement Initiative. Use the Model for Improvement to develop tracking and prevention measures that will move you toward ZERO preventable harm and death. Tools for tracking and best practices for eliminating UE can be downloaded from the Patient Safety Movement Foundation (www.patientsafetymovement.org) or the Airway Safety Movement (www.airwaysafetymovement.org). These tools include a core data set and a set of Actionable Patient Safety Solutions.
Please commit to the coalition:
get your hospital to take aim at eliminating unplanned extubation.
Drew died a preventable death from the complications of airway management. However, he has inspired a large community of airway safety experts to take on this problem. Together the coalition is working to ensure that another preventable death, like Drew’s, never happens again.
Help us make Drew’s Death meaningful.
Take action, now. Get your hospital involved.
MAKE A COMMITMENT.
Contact:
Dr. Arthur Kanowitz, Airway safety Movement: [email protected]
Dr. Lauren Berkow, Society for Airway Management: [email protected]
Ariana Longley, Patient Safety Movement Foundation: [email protected]
