| Adapted from Special Feature on Pulse Oximeters: The invention that changed the paradigm of patient safety around the world. (LiSA (1340-8836) vol28 No3 Page237-308, 2021.03 (in Japanese)
Disclaimer: The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information. |
The pulse oximeter is currently one of the most indispensable devices in the medical world, like the electrocardiogram or the sphygmomanometer. Even in early spring, 2021, as SARS-CoV-2 is still killing thousands of people per day around the world, some local governments in Japan are reportedly providing pulse oximeters to COVID-19 patients who are not hospitalized and have to quarantine themselves at home.
It was indeed a great achievement to invent pulse oximetry, improve its accuracy, and miniaturize the pulse oximeter. All three aspects were essential for the pulse oximeter to become popular worldwide. In April 2020, Takuo Aoyagi, Ph.D., who was the first inventor of the pulse-type oximeter in the world, passed away to the great regret of his colleagues as well as everyone in the medical community who knew of his great achievements. The authors, Akio Yamanishi and Ikuto Yoshiya, and their colleagues, were competitors of Dr. Aoyagi and his team as they worked on the development and clinical application of pulse oximeters.
We dedicate the following brief history of the development of pulse oximetry and its clinical application to our good old rival, the late Dr. Takuo Aoyagi.
1. Background
In 1969, members of the research and development group of Minolta Camera watched the astronauts, Neil Armstrong and Buzz Aldrin, become the first humans on the moon1. They carried a high resolution exposure meter, Space Meter 1° aboard their spacecraft, Apollo 11. Earlier, in 1962, a Minolta Himatic Camera with a selenium photo cell photosensor was on board the spacecraft, Friendship 7, as Mr. John H. Glenn Jr. orbited the earth. Over the next decade, the photosensor evolved from a selenium photocell, to a cadmium sulfide (CdS) photocell, and then a silicone photodiode (SPD). In 1972, Masaichirou Konishi, who acted as a negotiator with NASA, returned to Japan from the USA. On his return, a new research institution was established in Sakai, Osaka, to develop industrial and medical measuring devices. The first medical device developed in the new institution was a photoelectric pulse wave meter (photoplethysmograph). It utilized a light emission diode (LED) and a silicone photodiode (SPD) to generate and analyze transmitted red light through the fingertip. Although the response time of SPD was far shorter than CdS, the device did not become popular in the medical field. This photoelectric pulse wave meter, however, turned out to be the precursor of the fingertip pulse oximeter, OXIMET-MET-1417.
In 1973, M. Takeda et al2 reported that the pulsatile wave obtained by the photoelectric measurement of light transmitted through the fingertip represented the fluctuation of the thickness of blood in accordance with pulsation. This was the moment that the Minolta team became aware of the possibility of developing a non-invasive device to measure arterial oxygen saturation.
The principle of Wood-type ear oximetry (Wood EH and Geraci JE, 19493) utilized the difference of absorption of transmitted light between when the earlobe was arterialized by warming and when it was made ischemic by pressing it with a translucent balloon. It occurred to Yamanishi and his colleagues that pressing and depressing the earlobe made a kind of pulsation. Having just developed a fingertip pulse-wave meter, they soon created an algorithm to obtain oxygen saturation of arterial blood. In short, the incidental light that travels across the fingertip is absorbed by arterial and venous blood as well as by the tissues of the fingertip (skin, muscle, bone, connective tissue). Assuming that pulsatile fluctuation of the transmitted light is caused solely by the inflow of arterial blood, hemoglobin oxygen saturation can be calculated by the mathematical subtraction of light absorption by fingertip tissues from whole light absorption when arterial blood is full. The Minolta team was more than excited in anticipating an entirely new type of in vivo oximetry, the first since Wood and Geraci. But a few weeks later, the team members were astonished and disappointed to find a paper by Aoyagi et al entitled “The improvement of ear-piece oximeter” in the Proceedings of the 1974 Spring Meeting of the Japanese Society of Medical Electronics and Biological Engineering4. Minolta made a patent application as soon as possible, but it turned out the original idea of pulse oximetry by Aoyagi was one year ahead of Minolta as was recorded in Aoyagi’s research notes5.
Aoyagi’s invention of the principle of pulse oximetry started when he was working on the development of a cardiac output measurement device using the dye dilution method. Aoyagi had noticed that the spectrophotometric dye dilution curve fluctuated with heartbeats. It was a kind of reversed thinking to utilize the pulse wave to estimate arterial oxygen saturation in a non-invasive manner. The authors feel proud of Aoyagi’s great invention originally conceived in Japan. We are also happy to have run a good race with Aoyagi and his colleagues at the same time.
2. Development of the Fingertip Pulse Oximeter (OXIMET-MET-1471, Minolta Camera, Co Ltd)
After the first patent application made by Minolta for the basic principle of pulse oximetry, Minolta made a more detailed patent application for an apparatus, including circuits, designed by T. Kisanuki and T. Majima. Calculation of oxygen saturation was made by a simple linear equation from light absorption at the wavelengths 805nm (isosbestic point) and 650nm6.
Although a light emission diode (LED) was used as the light source for the pulse wave meter, a halogen lamp was employed with the pulse oximeter because of a shortage of LED lights. Because of this, the light emission lamp was incorporated into the chassis of the instrument and incident/emission light traveled through a pair of fiberoptic paths. In 1977, this device was marketed as OXIMET-1471 (Fig. 1).

OXIMET Met 1471:
The light emitted by a light emission diode travels to the finger probe and the transmitted light is analyzed by a silicon photodiode mounted in the chassis. The incident and transmitted light travels to and from the chassis through the fiberoptics, respectively
3. Clinical Application of OXIMET
In 1977, one of the authors, I. Yoshiya, was consulted by the other author, A. Yamanishi, about the clinical applicability of OXIMET. Yoshiya was then working in the Intensive Care Unit (ICU) of Osaka University Hospital and jumped at the suggestion because ICU patients needed invasive arterial gas measurements too frequently. OXIMET seemed to have potential as a bed-side monitoring device in critically ill patients.
First, we (I. Yoshiya and Y. Shimada, et al) calibrated the instrument against the oxygen saturation measurements obtained from blood samples of ICU patients6. It seemed that the pulse oximeter tended to overestimate arterial oxygen saturation below 90%, compared with the oxygen saturation measured on blood samples with Radiometer OSM-2 (Fig 2). The Minolta and Osaka University team tested the hypothesis that the overestimation of oxygen saturation with the pulse oximeter was due to the multiple scattering of incident light by the blood corpuscles. K. Hamaguri (Minolta) devised a model cell to which blood or hemoglobin solution was pumped in and out by a rotary pump (Fig. 2). By using the device, the effect of multiple scattering was successfully compensated for, as was previously reported by Shimada et al7. The accuracy of measurements by OXIMET has been reported by Yoshiya et al6, 8, Suzukawa et al9, Nakajima et al10, and Sarnquist et al11. The 1980 report by Yoshiya et al has the honor of being the first publication in English to introduce pulse oximetry as reported by E. C. Jr. Pierce at the 34th E.A. Rovenstine Memorial Lecture. A. Fukunaga (Professor of Anesthesiology, UCLA, Harbor, at that time) informed Yoshiya about this lecture, but regretfully the latter failed to attend the plenary lecture.
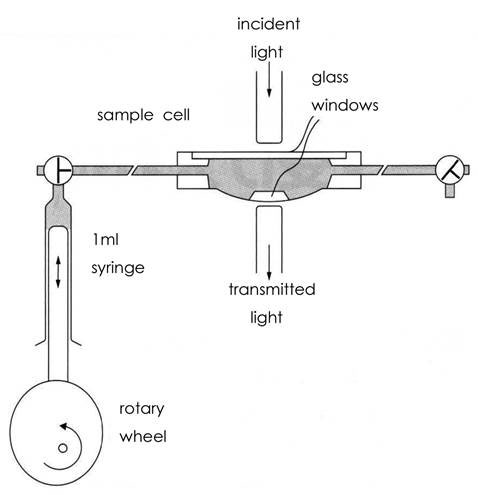
A pulse-generating apparatus for the in vitro pulse oximetry devised by Hamaguri:
A rotary pump generates pulse waves in an artificial cell with a pair of translucent glass windows on both sides of the cell. Light emitted by a halogen lamp travels across the windows. The transmitted light is spectrophotometrically analyzed for oxygen saturation by using the pulse oximetry principle. By changing the hematocrit of the sample blood pumped in the cell one can estimate the effect of scattering of light by blood corpuscles. Namely, the oxygen saturation by the in vitro pulse oximetry and that measured by a Radiometer (OSM-2) are compared with different hematocrit of the sample blood.
The authors utilized OXIMET as a safety monitor in the intensive care ward and in the operation theatre. It was also used as a monitor for patients with sleep apnea, but it could not be used routinely due to the size and weight of the finger-probe with fiberoptics.
4. Downsizing and Weight Reduction of Pulse Oximeters for Clinical Use
As stated above, the probe and fiberoptic cables of OXIMET were too large and heavy to be used as a bed-side monitor or a monitor for critically ill patients during emergency transportation. It was essential for both the finger probe and the amplifier to be downsized and made lighter to allow the pulse oximeter to be widely used in the clinical field. In 1981, Nellcor and Ohmeda, respectively, released pulse oximeters into the market with small finger probes utilizing LED and SPD. The pulse oximeter soon became popular in the United States, particularly in the operation theater. Several years later, the pulse oximeter was imported from the United States to its birth place, Japan.
Minolta also developed PULSOX-7 in 1987 that consisted of a finger probe using LED/SPD and a small, lightweight analyzer with a memory chip. This portable pulse oximeter was widely used for monitoring home oxygen therapy, sleep apnea, and transportation of critically ill patients. In 1990, PULSOX-7 climbed the summit of Mount Xixabangma (height: 8027m) carried by Akira Demizu, M.D. who was then a staff anesthesiologist at Osaka University Hospital. Demizu used to be a member of Kyoto University Alpine Club and joined the Kyoto University Medical Research Expedition to Xixabangma in 1990, to investigate the relationship between insomnia and arterial oxygen saturation at high altitude12. The successful Himalayan expedition of the pulse oximeter was attained by the ceaseless efforts of the Minolta team to attain size and weight reduction, energy saving, vibration resistance, ease of handling, and cost reduction13.
Aoyagi’s continuing effort to develop pulse oximetry was indeed admirable. He led the development team of Nihon Kohden to release OLV-1100/1200 into the market in 1987 and never stopped developing more accurate and motion-resistant pulse oximeters by adopting newer scattering theories and multiple-wavelengths to compensate for the scattering of light by blood corpuscles and body movement of the patient14. He gave a speech at the 34th Annual Meeting of the Japan Society of Technology in Anesthesia in commemoration of receiving the 2015 IEEE Medal for Innovations in Healthcare Technology. He said they had successfully settled the problem of body movement. Yamanishi remembers Aoyagi remarked in a chat with him “You’ll go and find pulse oximeters at supermarkets or electronic shops in the not-too distant future”. His prophecy has come to pass as of 2019-2021, in the pandemic of COVID-19.
Pulse oximetry was first invented by Aoyagi (Nihon Kohden), but there was competition from Minolta in Japan. The idea soon propagated to the United States where a device was produced using a smaller probe applicable for use in clinical settings. The improved pulse oximeter was imported back to Japan and was further improved and miniaturized. Currently, Konica-Minolta has a pulse oximeter weighing less than 40 grams, and pulse oximeters are routinely used on COVID-19 patients worldwide. The authors feel Aoyagi would have been happy about the internationalization of the development of the pulse oximeter.
Finally, we would like to express our sincere condolences to Dr. Aoyagi’s family.
Ikuto Yoshiya, Honorary Professor, Department of Anesthesiology, Osaka University Medical School
Akio Yamanishi, Former Chief, Medical Equipment Division, Minolta Camera Co. Ltd.
References
- Yamanishi A. The dawn of pulse oximeter. J Jpn Soc Med Instr 2005; 75:852– 62. (In Japanese)
- Takeda M, Shidara E, Atarashi J. Examination into calibration of photo plethysmography. Myakuha. 1973; 4:61-3. (In Japanese)
- Wood, EH, Geraci J E. Photoelectric determination of arterial oxygen saturation in man. J Lab Clin Med 1949; 34:387-401.
- Aoyagi T, Kishi M, Yamaguchi K, et al. Improvement of an earpiece oximeter. Abstracts. 13th Annual Meeting of Japanese Society for Medical and Biological Engineering, Osaka Japan. 1974; 90-1. (In Japanese)
- Aoyagi T. Invention of Pulse Oximetry and Later. Japanese Journal of Medical Electronics and Biological Engineering. 2011; 49:313-5 (In Japanese)
- Yoshiya I, Shimada Y, Tanaka K, et al. Spectrophotometric monitoring of arterial oxygen saturation in the fingertip. Med Biol Eng Comput 1980; 18: 27-32.
- Shimada Y, Yoshiya I, Oka N, et al. Effects of multiple scattering and peripheral circulation on arterial oxygen saturation measured with a pulse-type oximeter. Med Biol Eng Comput 1984; 22: 475-8.
- Yoshiya I, Shimada Y, Tanaka K, et al. A noninvasive in vivo oximeter. ICU & CCU 1978; 2: 455-60. (In Japanese)
- Suzukawa M, Fujisawa M, Matsushita F, et al. Use of pulse-type finger oximeter in anesthesia. J Anesthesia. 1978; 27: 600-5. (In Japanese)
- Nakajima S, Kubo Y, Samejima N, et al. Clinical application of a new (fingertip type) pulse wave oximeter. Jpn J Surg 1979; 41: 57-61. (In Japanese)
- Sarnquist FH, Todd C, Whicher C. Accuracy of a new non-invasive oxygen saturation monitor. Anesthesiology 1980; 53: S163.
- Demizu A. Matsubayashi K, Nakashima M, et al. High altitude insomnia and continuous pulse oximetry at night.Abstracts of the Seventh International Hypoxia Symposium, 1991, Alberta, Canada.
- Hamaguri K. Expansion of applications for pulse oximeters by reducing size and weight.J Jap Soc Med Instru 2005; 75: 868-72. (In Japanese)
- Aoyagi T, Fuse M, Ueda Y, et al. Improving precision of pulse oximetry. IAMPOV 2015; 11-3
| Read more articles from this special collection hosted by the APSF on Pulse Oximetry and the Legacy of Dr. Takuo Aoyagi. |
