Disclaimer: We aim to present letters from our readership that may generate further discussion on managing patients with COVID-19. Given the novelty of COVID-19, best-available clinical evidence is limited and supported from anecdotal reports from China, South Korea, Italy and other sites, and from studies of previous epidemics like SARS and MERS. The opinions expressed are those of the authors and not the APSF. These materials are presented for informational and educational purposes only and do not establish a standard of care or constitute medical or legal advice. The APSF does not support or endorse any specific idea, product, equipment, or trademarked technique. We strongly promote consistency with your governing bodies and organizations such as the CDC, WHO, ASA, AANA, and AAAA. Readers are reminded to consult with their institutions and medical/legal advisors regarding any of the views and opinions expressed by the authors.
| Related Article: Surgical Smoke Evacuators as a Method for Reducing Risk to Personnel of COVID-19 During Endotracheal Intubation and Extubation |
In the preceding Letter to The Editor of this publication, one of the authors communicated the concept of using an already widely available, ultra-high-efficiency-filtered operating room device, the Surgical Smoke Evacuator (SSE), placed near the patient’s face and airway, to divert and capture the aerosol and airborne load that is frequently produced during endotracheal intubation and extubation, and to thereby reduce the risk to healthcare workers (HCW’s) and nearby environment, surfaces and equipment.1
The SSE technique is compatible with and complementary to, nearly all intubation and extubation protocols and techniques that have been developed or suggested since the onset of the current COVID-19 pandemic, including using a clear plastic drape tented over the patient or rigid plastic “intubation boxes.”
The SSE technique can be conceptualized as an additional layer of personal protective equipment (PPE); or as another method of “source control” (similar to requiring all patients and HCW’s to wear facemasks at all times); or even as a miniaturized localized negative pressure respiratory isolation support system. The SSE technique should be considered as supplemental and additional to (and not a substitute for) the recommended appropriate PPE. It was also suggested that because of the widespread availability of SSE’s, and the high prevalence of COVID-19 due to community spread in many geographic areas, that this SSE technique could assist in moving toward a “universal precautions” approach to helping protect HCWs from aerosol- and airborne-generated pathogens during intubation and extubation.

Figure 1.
Simultaneously, the other author was utilizing and improving upon the plastic drape barrier technique by devising a simple arched plastic tubing frame which clamps to the operating room table at the level of the patient’s head to tent up the plastic drape. This gives the HCW performing the intubation or extubation, more space to work with their hands under the drape (see Figure 1).2
After realizing the potential additional value of utilizing a SSE under and in combination with the plastic drape, the effectiveness of: 1) the SSE technique, and of: 2) the combined SSE plus drape technique, was qualitatively tested in the laboratory using a smoke generator placed near the simulated patient’s face to simulate a visible aerosol load potentially created by intubation and extubation (see Figure 2). An SSE (Neptune 3, Stryker, Kalamazoo, MI, USA) was borrowed from the operating room and set on the 100% smoke evacuator setting (35 cu ft/min). 7/8-in diameter SSE tubing w/ a 3-1/2-in square plastic funnel at the end was placed on the simulated patient’s upper chest.
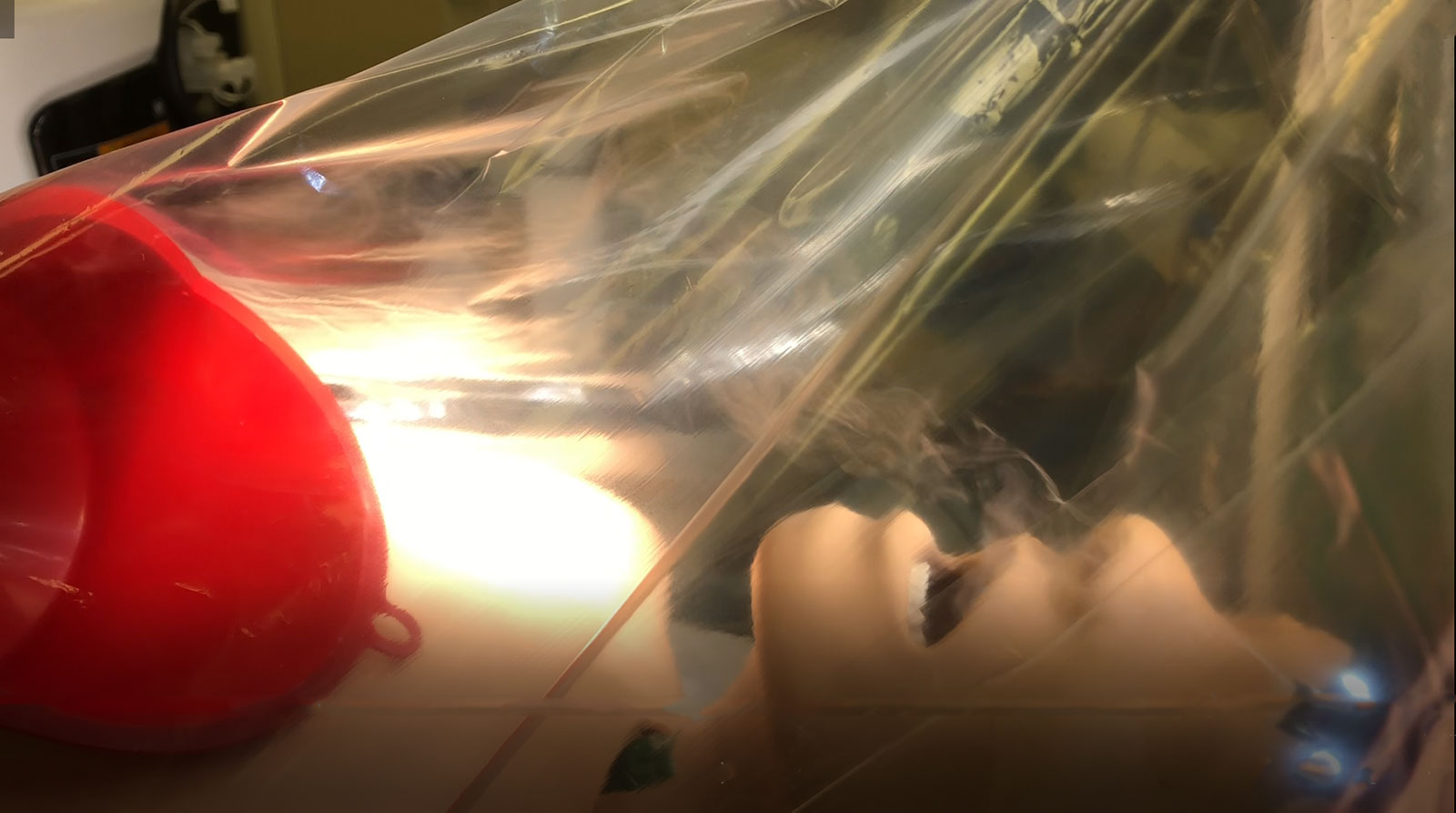
Figure 2. Depicts generated smoke being evacuated by the surgical smoke evacuator, under the plastic drape tent on a video clip captured by the authors.
The test qualitatively demonstrated that: 1) the SSE technique alone (without plastic drape) was fairly effective at diverting the simulated aerosol load (smoke) away from the head of the bed and capturing a moderate amount of the visible smoke, and that: 2) the combined SSE/plastic drape technique was highly effective at diverting and capturing the smoke and preventing accumulation of simulated aerosol load under the plastic drape.
The authors thus recommend the combined SSE/drape tent approach, or at least the SSE alone, as a routine additional COVID-19 risk reduction strategy during intubation and extubation for the protection of HCW’s and environment. Further research is required to definitively illustrate the efficacy of such a model in those being exposed to COVID-19.
Dr. Gonzalez is a Staff Anesthesiologist at Hackensack Meridian Southern Ocean Medical Center
Dr. Schaefer is the L.W.H. Blackman Endowed Chair for Patient Simulation and Research, and Professor of Anesthesiology and Perioperative Medicine at the Medical University of South Carolina
The authors have no conflict of interest.
References
- Gonzalez, RM. Surgical smoke evacuators as a method for reducing risk to personnel of COVID-19 during endotracheal intubation and extubation. APSF Newsletter online. Accepted for publication April 23, 2020. https://www.apsf.org
- Schaefer JJ, Gonzalez RM. Negative pressure intubation & extubation tent using disposable clear plastic sheeting and surgical smoke evacuator. https://youtu.be/n-5EXorJimg Accessed April 16, 2020
