Corneal abrasions are the most prevalent ocular injury seen in the postoperative period. Given the simplicity of treatment options for a simple corneal abrasion, a multidisciplinary joint protocol between the anesthesiology and ophthalmology departments at University of California Davis Medical Center was developed and implemented. This protocol has allowed anesthesiology professionals to successfully treat simple corneal abrasions in the postoperative anesthesia care unit and reduce the number of unnecessary ophthalmology consultations.
| Related Article: Letter to the Editor: Perioperative Corneal Abrasions from an Ophthalmologist’s Perspective |
 Corneal abrasions are the most prevalent ocular injury seen in the postoperative period.1,2 Corneal abrasions are painful and can be associated with blurred vision, tearing, redness, and a gritty sensation in the eyes,1,3 as well as more serious complications such as corneal scars and infections. In addition, they may be anxiety-provoking for the patient.4
Corneal abrasions are the most prevalent ocular injury seen in the postoperative period.1,2 Corneal abrasions are painful and can be associated with blurred vision, tearing, redness, and a gritty sensation in the eyes,1,3 as well as more serious complications such as corneal scars and infections. In addition, they may be anxiety-provoking for the patient.4
The cornea is one of the most highly innervated tissues in the body; hence, all corneal stimuli are perceived as painful.1 The clinical course of a corneal defect can range from an abrasion to more serious complications such as corneal ulcerations or erosions, which can result in long-term consequences like vision loss.5
In addition to the pain and discomfort, patients with corneal abrasions may also experience delayed discharge from the Postanesthesia Care Unit (PACU) as they await an ophthalmology consultation. Given the simplicity of treatment options for an uncomplicated corneal abrasion, which typically involve a combination of eye drops,6 we developed and implemented a multidisciplinary joint protocol between the anesthesiology and ophthalmology departments at the University of California (UC) Davis Medical Center.
Prior to the development and implementation of our protocol, there was often uncertainty on how to diagnose and manage simple corneal abrasions, which would lead to unnecessary ophthalmology consultations, prolonged PACU length of stay, and, ultimately, decreased patient satisfaction. Our goal was to streamline the management of corneal abrasions in the PACU at UC Davis Medical Center, reduce the number of ophthalmology consultations, and improve patient satisfaction.
When a patient complains of eye pain or blurry vision in the PACU, the protocol calls for the PACU nurse to call the anesthesiology resident to perform an eye exam (Figure 1). The resident comes to the bedside to assess for vision changes, redness, tearing, photophobia, or a gritty sensation. At this point, if the patient reports vision loss, ophthalmology is consulted. If there is no vision loss, the examination continues with the anesthesiology resident administering fluorescein stain to the affected eye and examining it with the cobalt blue light from the ophthalmoscope, both of which are available in the PACU. If no corneal defect is present, the likely diagnosis is keratoconjunctivitis sicca (dry eyes), and artificial tears can be ordered for treatment. If a corneal defect is present, then the likely diagnosis is a corneal abrasion, and erythromycin ointment is ordered for the patient, which is administered every 4 hours until symptoms resolve. If symptoms persist for greater than 24 hours, the patient should be seen by the ophthalmology service if still an inpatient or in clinic if discharged. Every patient with a corneal abrasion is provided with the ophthalmology clinic number for follow-up.
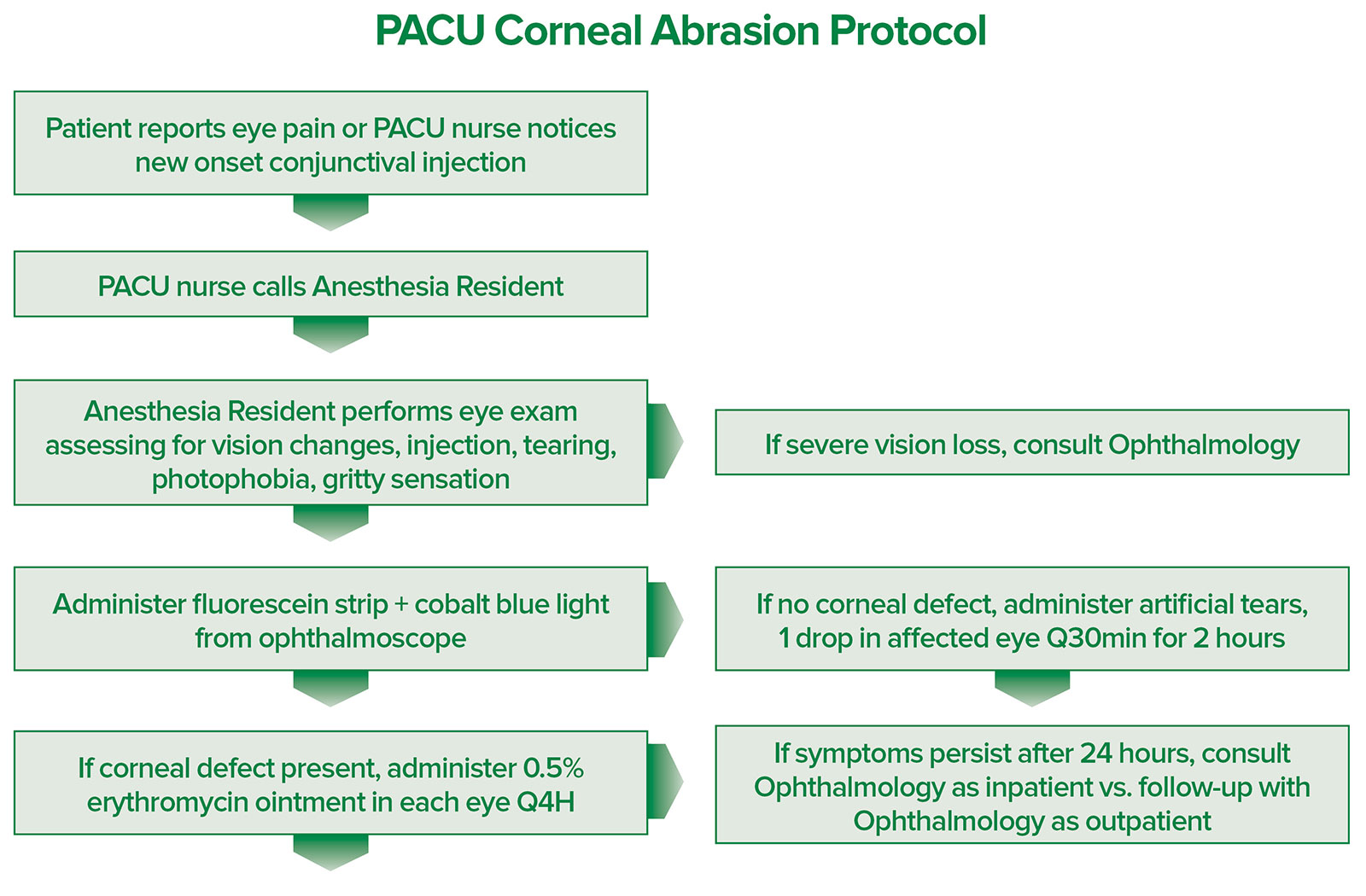
Figure 1: The University of California Davis PACU Corneal Abrasion Protocol. This is a step-wise protocol to streamline the management of corneal abrasions in the PACU. PACU: Postanesthesia Care Unit.
This protocol was officially implemented in the UC Davis Medical Center PACU in January 2019. To track the corneal abrasions that occurred in the PACU, a corneal abrasion patient list was developed on the Epic electronic medical record, and any patient with a diagnosis of corneal abrasion was added to this list. Prior to the development of the protocol, it was challenging to keep track of corneal abrasions that occurred in the PACU, and only a handful were reported over years. With the development of the protocol, these cases have been readily reported and tracked. The following parameters were assessed: number of ophthalmology consultations, resolution of symptoms, and any follow-up phone calls or office visits with reported ocular complications.
Our data on corneal abrasions in the PACU spans from July 2017 to November 2025, with the implementation of the protocol in January 2019. Pre-intervention data availability was from July 2017 through December 2018. Post-intervention data availability was from January 2019 to November 2025. A total of 121 patients were included in the data analysis, all of whom had a diagnosis of corneal abrasion in the PACU. Of the 121 patients, 17 were pre-intervention and 104 were post-intervention. Of the 17 cases that occurred prior to the protocol, 14 cases (82.35%) had an ophthalmology consultation. In contrast, of the 104 cases that occurred after the protocol, only 9 (8.6%) had an ophthalmology consultation (Figure 2). Per a two-proportion z-test, when the number of consultations were compared between the two time periods, there was a significant decrease (p-value of <.001) in the number of ophthalmology consultations.
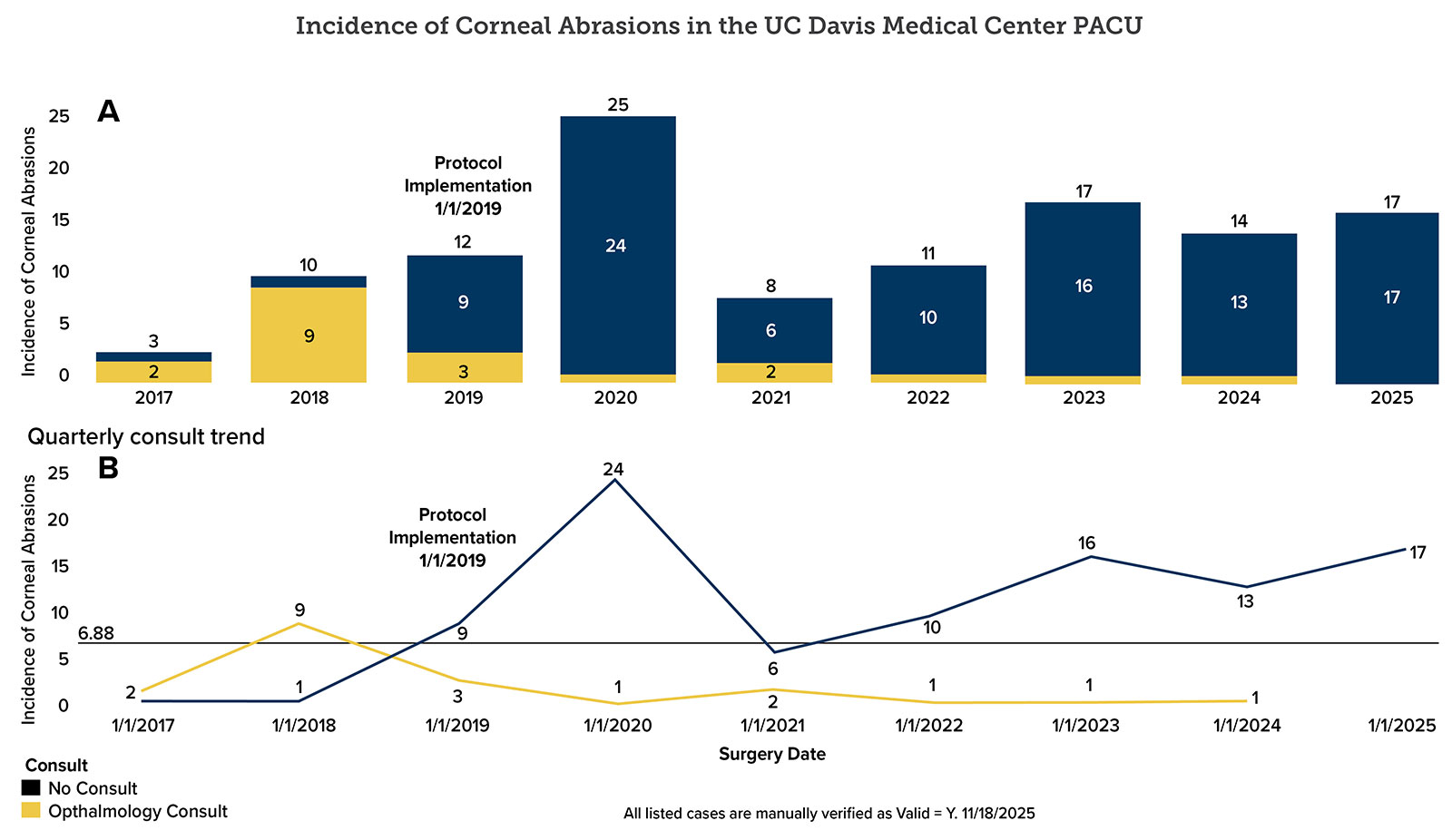
Figure 2: The incidence of corneal abrasions in the UC Davis Medical Center PACU. A) Bar chart demonstrating number of abrasions. The number on top represents the total number of abrasions, while the number in the bar represents the number of consults. B) Quarterly consult trend. UC: University of California; PACU: Postanesthesia Care Unit
Our data review shows that all patients that were treated with the protocol had complete resolution of symptoms and there were no reported complications, as determined by follow-up phone calls or follow-up office visits. These findings are reassuring and indicate that our protocol has proven to be effective in diagnosing and managing corneal abrasions in the PACU. The complete resolution of symptoms, in the absence of ocular complications, likely enhanced patient satisfaction.
Prior to the initiation of the protocol, there was a great deal of uncertainty among practitioners regarding the management of corneal abrasions. Since the implementation of the PACU Corneal Abrasion protocol, anesthesia teams have been able to successfully diagnose and manage simple corneal abrasions in the PACU. This protocol has now been in use in the UC Davis Medical Center PACU for over five years with great success and positive feedback from the anesthesiology faculty and residents. The number of unnecessary ophthalmology consultations has significantly decreased and all patients had complete resolution of their symptoms with no reported long-term postoperative ocular complications.
During the evaluation period, 95 cases of corneal abrasion were successfully managed by anesthesiology clinicians without requiring ophthalmology involvement. Based on the institution’s average ophthalmology consult charge of $482 per case, these eliminated consults translated into an estimated $46,000 in total patient cost savings. This outcome demonstrates that an evidence-based, anesthesiology-led approach to managing perioperative corneal abrasions can reduce unnecessary specialty consults, streamline patient care, and yield meaningful financial benefits for the hospital system.
This protocol has ultimately allowed for a more streamlined management of corneal abrasions in the UC Davis Medical Center PACU. There has been a statistically significant reduction in the number of unnecessary ophthalmology consultations, complete resolution of patient symptoms, and no reported permanent ocular complications.
Reihaneh Forghany, MD, FASA, is an assistant professor of anesthesiology at the University of California, Davis Medical Center, Sacramento, CA.
The author reports no conflicts of interest.
REFERENCES
- Malafa MM, Coleman JE, Bowman RW, Rohrich RJ. Perioperative corneal abrasion: updated guidelines for prevention and management. Plast Reconstr Surg. 2016;137:p790e–798e. PMID: 27119941.
- White E, Crosse MM. The aetiology and prevention of peri-operative corneal abrasions. Anaesthesia. 1998;53:157–161. PMID: 9534639.
- Wilson SA, Last A. Management of corneal abrasions. Am Fam Physician. 2004; 70:123–128. PMID: 15259527.
- Yu HD, Chou AH, Yang MW, Chang CJ. An analysis of perioperative eye injuries after nonocular surgery. Acta Anaesthesiol Taiwan. 2010; 48:122–129. PMID: 20864060.
- Ahmed F, House RJ, Feldman BH. Corneal abrasions and corneal foreign bodies. Prim Care. 2015;42:363–375. PMID: 26319343.
- Segal KL, Fleischut PM, Kim C, et al. Evaluation and treatment of perioperative corneal abrasions. J Ophthalmol. 2014;2014:901901. PMID: 24672709.
