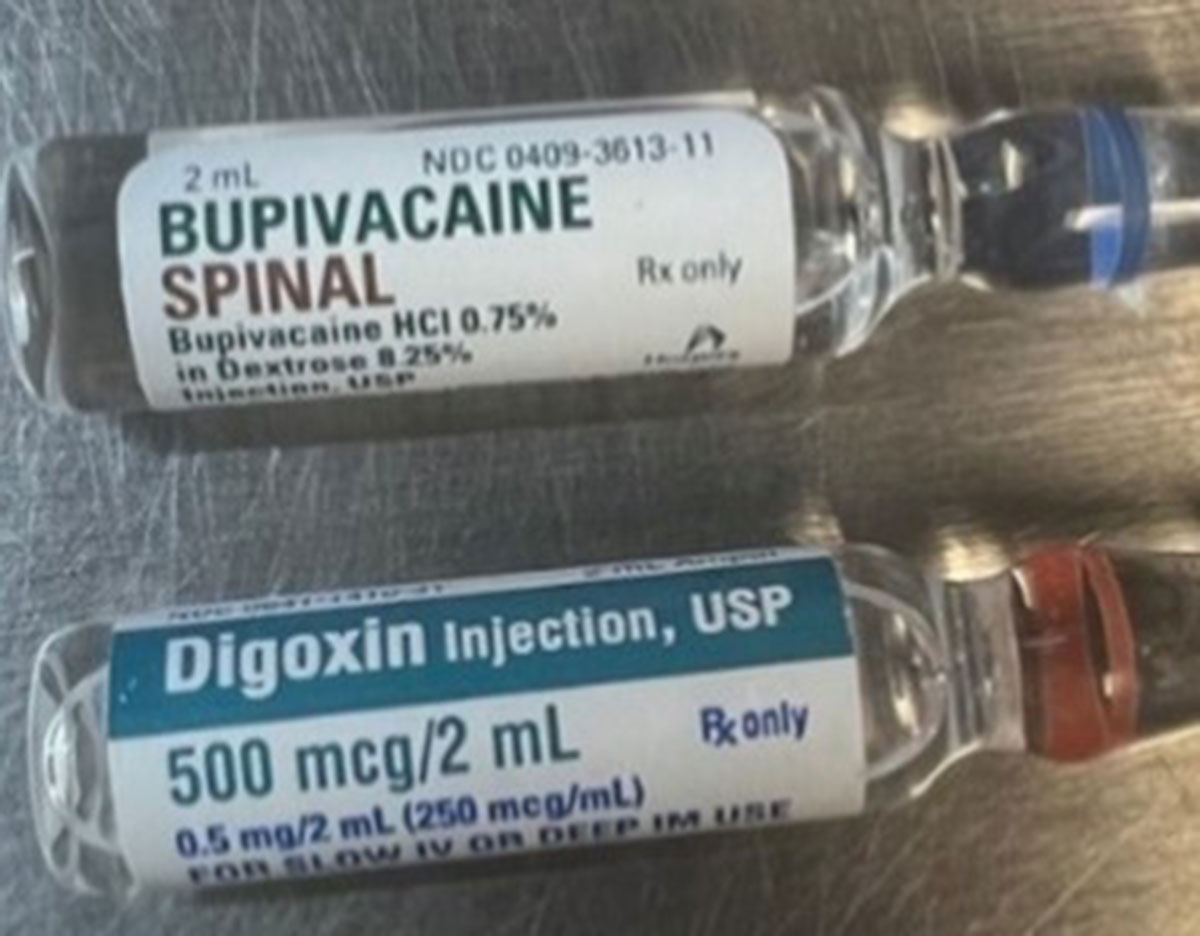
Examples of ampules of BUPivacaine Spinal by Hospira (NDC 0409-3613-11) (top) and digoxin by Hikma Pharmaceuticals (NDC 0641-1410-31) (bottom).
The Institute for Safe Medication Practices (ISMP) published a featured article “Obstetrical Patient Receives Ampule of Digoxin Instead of BUPivacaine for Spinal Anesthesia” highlighting a medication error and safe practice recommendations.
- A pregnant patient died after an anesthesia professional mistakenly administered digoxin instead of BUPivacaine during a cesarean delivery.
- BUPIVACAINE SPINAL and digoxin are both available in 2 mL ampules, which can heighten the risk of mix-ups between the two drugs.
- A review of 33 inadvertent neuraxial cardiovascular medication administration errors between 1972 and 2022 found digoxin was the medication most commonly administered in error and was associated with paraplegia and encephalopathy in eight patients.
ISMP makes several recommendations, including:
- The FDA should take steps to have manufacturers package digoxin in vials.
- Organizations should review which medications are available in each unit-specific ADC location, anesthesia tray, and medication kit.
- Evaluate whether digoxin needs to be stocked in your OR and labor and delivery unit or if it can be requested from the pharmacy, as needed.
- Employ individual locked pockets or segregated storage, especially for high-alert medications like digoxin.
For more recommendations and information visit:
