ISMP Alert Republished with Permission: https://home.ecri.org/blogs/ismp-alerts-and-articles-library/manufacturer-s-dexmedetomidine-premixed-iv-bags-may-be-packaged-within-an-overwrap-labeled-as-acetaminophen
A Hikma product with an overwrap labeled acetaminophen injection 1,000 mg/100 mL (NDC 0143-9386-01, lot number 24070381, expiration date 09/2025) (Figure 1), may contain a dexmedeTOMIDine 400 mcg/100 mL infusion bag (lot number 24070461, expiration date 03/2026) with Canadian labeling, a different font, and follows ISMP Canada’s tall man lettering (i.e., dexmedeTOMidine) (www.ismp.org/ext/1394) which is different from the tall man lettering (i.e., dexmedeTOMIDine) on the ISMP List of Look-Alike Drug Names with Recommended Tall Man (Mixed Case) Letters (www.ismp.org/node/136) (Figure 2).
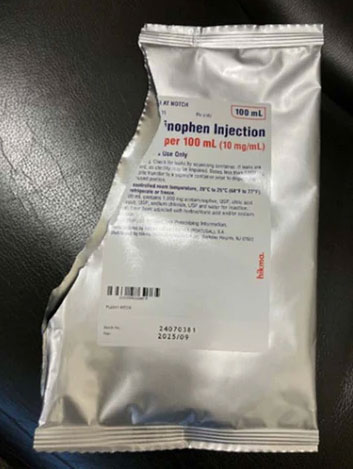
Figure 1. Hikma’s overwrap labeled acetaminophen injection 1,000 mg/100 mL may contain an infusion bag labeled dexmedeTOMidine 400 mcg/100 mL.
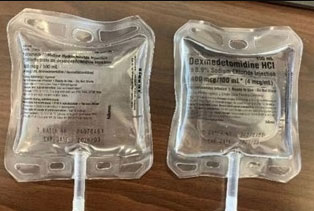
Figure 2. An infusion bag (left) found inside the acetaminophen injection overwrap by Hikma, was labeled dexmedeTOMidine 400 mcg/100 mL with Canadian labeling and a different font compared to the US product labeling (right).
An event was reported to ISMP where a nurse removed what she thought was an acetaminophen 1,000 mg/100 mL infusion bag from the automated dispensing cabinet (ADC), scanned the barcode on the overwrap, and administered the infusion to the patient. Approximately 15 minutes later, the patient experienced bradycardia and bradypnea. The nurse looked at the empty bag hanging on the intravenous (IV) pole and discovered that it was labeled “dexmedeTOMidine hydrochloride injection, 400 mcg/100 mL.” The nurse notified the prescriber and provided supplemental oxygen to the patient. Fortunately, the patient recovered.
We have reached out to the US Food and Drug Administration (FDA) and Hikma to notify them of this concern. Hikma told us they are conducting an immediate and ongoing investigation. They have notified the impacted wholesalers who have placed Hikma’s acetaminophen 1,000 mg/100 mL injection with the lot number 24070381 in quarantine. A formal recall is planned. If your organization has purchased this product, check your inventory, and if an infusion bag overwrap labeled as acetaminophen with lot number 24070381 is found, sequester the product until further instructions are provided by the FDA/wholesaler. While this is an unusual situation, the best practice is to scan the barcode directly on an infusion bag (not the overwrap) prior to administration. Educate staff to read the infusion bag labels prior to barcode scanning and administration, and to be vigilant when checking the actual infusion bag for Hikma’s acetaminophen injection, regardless of the lot. Report issues to ISMP (www.ismp.org/report-medication-error), FDA (www.ismp.org/ext/544), and the manufacturer (www.ismp.org/ext/1395).
The National Alert Network (NAN) is a coalition of members from the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP). The network, in cooperation with the Institute for Safe Medication Practices (ISMP) and the American Society of Health-System Pharmacists (ASHP), distributes NAN alerts to warn healthcare providers about the risk of medication errors that have caused or may cause serious harm or death, or to warn them about new findings that could cause harm and/or are being reported with unusual frequency. NCC MERP, ISMP, and ASHP encourage the sharing and reporting of medication errors both nationally and locally, so that lessons learned can be used to increase the safety of the medication-use system.
