Teamwork is an essential component of patient safety in perioperative medicine. Its successful use in the operating room depends on leadership, situational awareness, team orientation, adaptability, and backup behavior. Teamwork may be facilitated by different training methodologies including comprehensive techniques, brief team training and quality improvement initiatives. Each of these approaches has its own strengths and weaknesses.
INTRODUCTION
 On a warm summer Saturday at University Hospital in Newark, NJ, a patient arrived in the operating room profusely bleeding from a gunshot wound to the abdomen. A massive transfusion protocol was activated and rapid infusion of blood products was initiated as the surgeons raced to repair severe injuries to the kidneys, spleen, and liver. However, soon after the case began, unforeseen problems, unrelated to the patient’s clinical condition, arose. First, the rapid infuser overheated and started alarming loudly, endangering the patient’s resuscitation. The anesthesia team immediately switched the infusions to peripheral lines and retrieved another rapid infuser to resume resuscitation. A short time later, the hum of the anesthesia equipment suddenly went silent; power to half of the operating room terminated without warning. One trainee retrieved a portable, battery-powered monitor while another trainee connected a bag-mask apparatus to an oxygen tank, manually ventilating the patient (the backup battery on the anesthesia workstation also failed). The attending plugged all needed anesthesia devices into the remaining working power outlets located on the opposite side of the room. Monitoring and ventilation were maintained as maintenance crews worked to restore power to the rest of the room. Later, during transport to the intensive care unit, an anxious medical student pushed the bed too quickly, dislodging a peripheral intravenous (IV) catheter from the patient’s arm. As the patient bled onto the bed, a resident ran back to the operating room to retrieve gauze and IV supplies, while another resident switched the infusions to a working intravenous line. The attending anesthesiologist continued to manually ventilate the patient, while troubleshooting oxygen desaturation caused by a loss of suction from the chest tube (dropping as low as 80% while suction was restored).
On a warm summer Saturday at University Hospital in Newark, NJ, a patient arrived in the operating room profusely bleeding from a gunshot wound to the abdomen. A massive transfusion protocol was activated and rapid infusion of blood products was initiated as the surgeons raced to repair severe injuries to the kidneys, spleen, and liver. However, soon after the case began, unforeseen problems, unrelated to the patient’s clinical condition, arose. First, the rapid infuser overheated and started alarming loudly, endangering the patient’s resuscitation. The anesthesia team immediately switched the infusions to peripheral lines and retrieved another rapid infuser to resume resuscitation. A short time later, the hum of the anesthesia equipment suddenly went silent; power to half of the operating room terminated without warning. One trainee retrieved a portable, battery-powered monitor while another trainee connected a bag-mask apparatus to an oxygen tank, manually ventilating the patient (the backup battery on the anesthesia workstation also failed). The attending plugged all needed anesthesia devices into the remaining working power outlets located on the opposite side of the room. Monitoring and ventilation were maintained as maintenance crews worked to restore power to the rest of the room. Later, during transport to the intensive care unit, an anxious medical student pushed the bed too quickly, dislodging a peripheral intravenous (IV) catheter from the patient’s arm. As the patient bled onto the bed, a resident ran back to the operating room to retrieve gauze and IV supplies, while another resident switched the infusions to a working intravenous line. The attending anesthesiologist continued to manually ventilate the patient, while troubleshooting oxygen desaturation caused by a loss of suction from the chest tube (dropping as low as 80% while suction was restored).
When the patient was successfully transferred to the SICU, the team marveled at the ease with which three potentially catastrophic iatrogenic complications were rapidly managed. Timely communication, quick coordination of tasks, and dedication to patient safety led the team to act quickly so that patient care was not compromised despite equipment failure, power failure, and logistical challenges during transport.
During crisis situations, the quality of teamwork amongst healthcare professionals may be the determining factor for successful patient care. Knowing what factors contribute to a well-functioning team and practicing these critical skills will better prepare all anesthesia professionals for the inevitable crises we will face. In this article, we discuss the various aspects of teamwork that were crucial in the care of a critically ill trauma patient when several unforeseen challenges arose.
TEAMWORK & PATIENT SAFETY
The “big five” components of successful teamwork are leadership, situational awareness, team orientation, adaptability, and backup behavior (Table 1).1 These behaviors are rooted in dynamic evaluation of the situation, communication, re-assessment, task allocation, and collaboration between team members.
Table 1. The “Big Five” components of teamwork, associated definitions, and how they apply to the case discussed.1
| Teamwork components | Definition | Application to case |
| Directive Leadership | Direct and coordinate activities of the team, assign tasks, assess performance, provide psychological safety, update team knowledge | Anesthesiology attending led patient care throughout the unforeseen challenges and continually evolving situation |
| Situational awareness (also known as mutual performance monitoring) | Develop common understanding of the changing team environment and apply strategy to tackle new challenges | Prompt realization that electrical power had failed, with subsequent quick retrieval of battery-powered monitor and bag-mask aparatus as the first life-saving steps |
| Team Orientation | Take team members’ strengths into account during group interaction and prioritizing team’s goal over individual goals. | Anesthesia resident recognized PIV was dislodged during transport; one resident got supplies to start another IV while the second resident switched active infusions to another line |
| Adaptability | Adjust based on new information or changing conditions, shifting workload, and reallocating resources | Faculty and resident infused blood products through PIV while others obtained a new rapid infuser from cardiac OR |
| Backup Behavior | Anticipate others’ needs and shift workload or change responsibilities | Co-ordinated efforts between anesthesia providers and technician quickly identified the emergency power outlets to restore power to workstation and Pyxis |
| Adapted from Salas E, Sims DE, Burke CS. Is there a “Big Five” in Teamwork? Small Group Research. 2005;36(5):555-599. doi:10.1177/1046496405277134. | ||
While clinicians recognize the degree to which strong teamwork contributes to successfully navigating a crisis, the effect of teamwork on the successful care of a patient may be difficult to directly ascertain. Research in this arena often focuses on retrospective observation, trials using simulation, or other educational interventions. A prospective observational study found a strong correlation between the occurrence of errors during cardiac surgery and failure in teamwork, and another showed that patients had a higher risk of death when good communication behaviors, especially during hand-offs, were less frequent.2,3 In simulation of an obstetric emergency, an association was found between improved teamwork (based on a generic teamwork score) and decreased time to effective clinical intervention.4 These effects were statistically significant and large effects have been found in multiple other studies of team processes’ effect on clinical performance.5
Nonetheless, understanding these principles is not enough to ensure well-functioning teams. Reinforcing these ideas through team training, especially simulation, is recommended by the Agency for Healthcare Research and Quality (AHRQ) to increase patient safety.6 As anesthesia professionals, we often function in ad hoc teams that do not have the luxury of time to develop mutual trusting relationships prior to patient care. By practicing Crisis Resource Management in simulation or TeamSTEPPS, anesthesia professionals may develop the skillset needed to lead an ad hoc team.7,8
Improvement in teamwork in the healthcare setting may be advanced using three different methods, with pros and cons of each (See Figure 1).9 Comprehensive, but generic, curricula, such as the aforementioned TeamSTEPPS framework, are widely available. However, they are time and labor intensive, may not be applicable to particular healthcare settings (since they were first developed in aviation), and may not directly translate to improving patient outcomes.
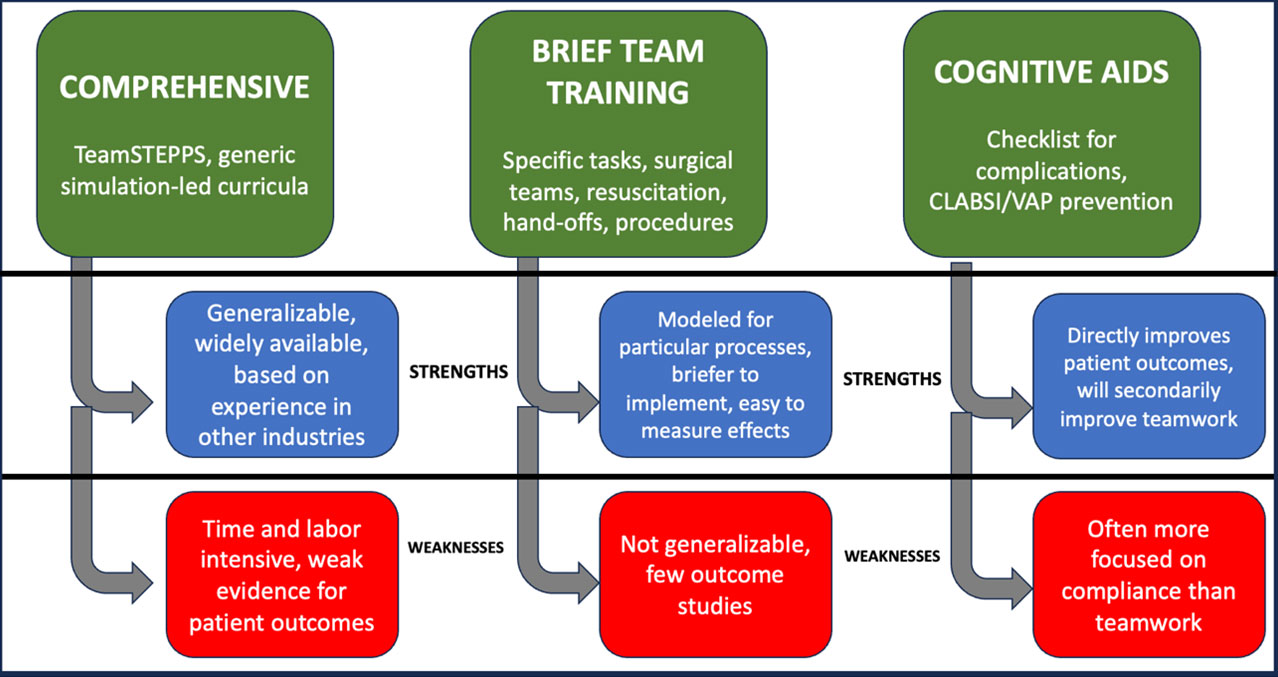
Figure 1. Three team training methods and their associated strengths and weaknesses.
Another team-training modality is brief team training for specific healthcare tasks and activities. This method is often used for team training for specific surgeries, resuscitation during code situations, hand-offs, or procedures. The advantage of this type of training is that it is brief and easier to utilize than a comprehensive model; however, the teamwork modeled therein is not broadly applicable for the participants.
The third educational framework involves cognitive aids that facilitate teamwork by involving required personnel. This includes checklists for patient care handoff, handling perioperative complications, and prevention of central line associated blood stream infections or catheter associated urinary tract infections. This training supports improved patient outcomes, but may be more focused on compliance with regulatory bodies than specifically improving teamwork among healthcare practitioners.10
Clinical personnel credited several crucial elements with the success of the patient care and their ability to navigate multiple unrelated crises. These factors included simulation education, which is incorporated very early into training and often covers difficult scenarios such as complex trauma surgery. Task-specific training, which has been accomplished via multi-disciplinary and inter-departmental training sessions with nursing and surgery, was also cited as a contributing factor towards success. This type of training, even on an unrelated task (e.g. malignant hyperthermia or cardiopulmonary arrest), created an atmosphere in which clinicians felt comfortable asking for help and assigning themselves into relevant and active roles. Situational awareness, and timely communication of the consequences of changes in the environment, facilitated the identification of tasks for completion by group members. Finally, adaptability is a crucial skill that helps clinicians develop and deploy contingency plans quickly when faced with new challenges to the team’s function.
RECOMMENDATIONS FOR ANESTHESIA PROFESSIONALS
Education in teamwork skills should begin in training and continue throughout a clinician’s career. Each anesthesia department should invest in improving providers’ ability to work in a clinical team in multiple situations, including caring for patients in the operating room, addressing perioperative efficiency, tackling and confronting adverse events, or improving quality of care.
Good teamwork can guide the successful navigation of stressful patient encounters in perioperative medicine. However, teamwork should also be viewed as an essential component of a well-functioning anesthesia department in all aspects of patient care. Working to improve teamwork at all times ensures that a well-functioning team will perform required actions in an effective and timely manner to prevent, identify and address potential patient safety events. While the profession of anesthesiology may appear to those unfamiliar with the operating room as an individual or solo practitioner specialty, teamwork is an essential component of perioperative efficiency and patient safety, and can mitigate or even prevent future adverse events.
George Tewfik is an associate professor in the Department of Anesthesiology at Rutgers-New Jersey Medical School, Newark, New Jersey, USA.
Uma Munnur is a professor of anesthesiology at Baylor College of Medicine, Houston, Texas, USA.
Candace Chang is an associate professor of Anesthesiology at University of Utah, Salt Lake City, Utah, USA.
Giovanna Patafio is a resident anesthesiologist at Rutgers-New Jersey Medical School, Newark, New Jersey, USA.
Esther Masilamony is a resident anesthesiologist at Rutgers-New Jersey Medical School, Newark, New Jersey, USA.
The authors have no conflict of interest.
REFERENCES
- Salas E, Sims DE, Burke CS. Is there a “Big Five” in Teamwork? Small Group Research. 2005;36(5):555-599. doi:10.1177/1046496405277134
- ElBardissi AW, Wiegmann DA, Henrickson S, Wadhera R, Sundt TM, III. Identifying methods to improve heart surgery: an operative approach and strategy for implementation on an organizational level. European Journal of Cardio-Thoracic Surgery. 2008;34(5):1027-1033. doi:10.1016/j.ejcts.2008.07.007
- Mazzocco K, Petitti DB, Fong KT, et al. Surgical team behaviors and patient outcomes. Am J Surg. May 2009;197(5):678-85. doi:10.1016/j.amjsurg.2008.03.002
- Siassakos D, Fox R, Crofts JF, Hunt LP, Winter C, Draycott TJ. The management of a simulated emergency: better teamwork, better performance. Resuscitation. Feb 2011;82(2):203-6. doi:10.1016/j.resuscitation.2010.10.029
- Schmutz J, Manser T. Do team processes really have an effect on clinical performance? A systematic literature review. Br J Anaesth. Apr 2013;110(4):529-44. doi:10.1093/bja/aes513
- Wacker J, Kolbe M. Leadership and teamwork in anesthesia – Making use of human factors to improve clinical performance. Trends in Anaesthesia and Critical Care. 2014/12/01/ 2014;4(6):200-205. doi:https://doi.org/10.1016/j.tacc.2014.09.002
- Murray WB, Foster PA. Crisis resource management among strangers: principles of organizing a multidisciplinary group for crisis resource management. J Clin Anesth. Dec 2000;12(8):633-8. doi:10.1016/s0952-8180(00)00223-3
- Buljac-Samardzic M, Doekhie KD, van Wijngaarden JDH. Interventions to improve team effectiveness within health care: a systematic review of the past decade. Hum Resour Health. Jan 8 2020;18(1):2. doi:10.1186/s12960-019-0411-3
- Thomas EJ. Improving teamwork in healthcare: current approaches and the path forward. BMJ Quality & Safety. 2011;20(8):647-650. doi:10.1136/bmjqs-2011-000117
- Haugen AS, Sevdalis N, Søfteland E. Impact of the World Health Organization Surgical Safety Checklist on Patient Safety. Anesthesiology. Aug 2019;131(2):420-425. doi:10.1097/aln.0000000000002674
