INTRODUCTION
The photodynamic bone stabilization system (PBSS) is an alternative to traditional orthopedic surgical options that uses a photosensitive monomer to fill a reamed bony canal and stabilize fractures or impending fractures.1 This minimally-invasive procedure provides immediate stability, allows for early mobility and weight-bearing, and can reduce the risk of complications associated with traditional fracture treatment methods.2 As such, PBSS can be beneficial for high-risk patients who may not withstand traditional operative interventions, including older patients with multiple comorbidities, including metastatic cancer.1
Potential complications following the PBSS procedure include the dislodgement of the PBSS debris, or monomer or fat embolus from the bone’s medullary canal,3 resulting in serious cardiopulmonary effects, including pulmonary embolism (PE), right ventricular (RV) failure and cardiac arrest. Thus, while the PBSS procedure is minimally invasive and generally safe, patients with advanced cardiopulmonary disease may not tolerate intraoperative complications such as PE, and swift recognition and intervention can prevent catastrophic cardiopulmonary collapse.
CASE DESCRIPTION
We present a case of a 68-year-old female who underwent prophylactic stabilization of the right humerus using PBSS. The patient’s medical history was significant for metastatic leiomyosarcoma to the right humerus that had progressed over the previous two years with new findings of multiple metastatic pulmonary nodules on computed tomography. Additionally, there was concern for an impending fracture of the right humerus. The patient also had a history of deep venous thrombosis and PE, and apixaban was held for two days prior to surgery. Preoperative evaluation was notable for transthoracic echocardiography demonstrating normal left ventricular (LV) function and ejection fraction, mildly reduced RV function, and an estimated RV systolic pressure of 66.1 mmHg, consistent with severe pulmonary hypertension.
Following induction of general anesthesia, intubation, and placement of a left radial arterial catheter, the procedure progressed without incident for approximately two hours. However, following the bone reaming and subsequent balloon inflation steps of the PBSS procedure, the patient experienced sudden cardiopulmonary collapse characterized by severe hypoxemia (oxygen saturation of 40-50%), profound hypotension (blood pressure of 39/33 mmHg), and bradycardia (heart rate reduced to 14 beats per minute) with non-palpable pulses.
Cardiopulmonary resuscitation was initiated, achieving return of spontaneous circulation after several rounds of advanced cardiac life support. Transesophageal echocardiography (TEE) revealed a massively dilated RV and a small, underfilled, hyperdynamic LV, suggestive of a large PE (Figure 1). Despite aggressive resuscitation efforts, RV function continued to deteriorate, necessitating the initiation of emergent veno-arterial extracorporeal membrane oxygenation (VA-ECMO) via femoral access.
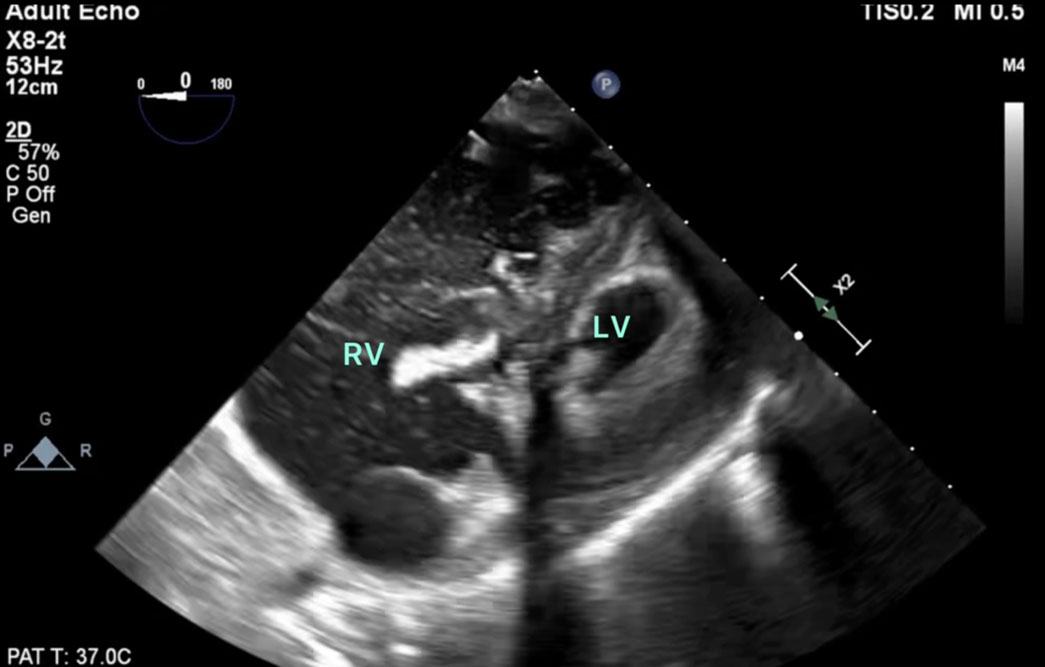
Figure 1. Trans-gastric basal short-axis view reveals a dilated right ventricle containing multiple hyperechoic shadows consistent with the appearance of emboli, and a severely underfilled and hyperdynamic left ventricle.
Postoperatively, the patient was initially awake and neurologically intact. However, on the fifth postoperative day, she developed an intracranial hemorrhage. Given significant neurological decline and the underlying aggressive cancer diagnosis, the decision was made to transition the patient to comfort care.
DISCUSSION
PBSS is a minimally invasive technique that is an alternative to traditional orthopedic surgical options and involves several stages. First, canal preparation is performed by reaming of the bone canal over a guidewire. Next, a balloon catheter is inserted into the medullary canal. The balloon is then infused with a photosensitive monomer that expands under pressure to fill the canal to attain a press-fit against the intact cortices. Finally, a fiberoptic blue light is introduced to induce polymerization and solidification of the monomer.1,4,5
PBSS, while innovative and potentially risk-reducing, is associated with several complications including fat, debris, and polymer embolization. Two cases specifically describe severe hemodynamic collapse during humerus stabilization with photodynamic implants.5 In both cases, hemodynamic instability occurred shortly after balloon dilation and infusion of monomer into the space. Both patients developed acute hypoxic respiratory failure and required high inspired oxygen levels for several days postoperatively.
In our patient, the indication for PBSS was impending rather than a completed pathologic fracture. In a completed pathologic fracture, an increase in medullary pressure during monomer infusion might be relieved through the fracture site itself, functioning like a “pop-off” valve. When managing cases for an impending fracture, the intact medullary canal may instead function as a closed system, leading to greater pressurization during balloon inflation.6 Despite the prophylactic creation of a distal vent hole intraoperatively to mitigate the intramedullary pressure during balloon inflation in our case, the medullary contents (including a combination of coagulated blood and bone particles following reaming) were likely directed towards the endosteal vessels and entered the systemic circulation, resulting in PE and cardiovascular collapse.
Patients undergoing PBSS frequently have underlying comorbidities that can increase the risks of this procedure (Figure 2). Older patients (a common demographic of patients undergoing PBSS) have an increased risk of pulmonary hypertension due to the cumulative effects of various age-related risk factors and comorbidities, such as left heart disease, chronic lung disease, thromboembolic disease, and progressive stiffening of the pulmonary arteries. Older adults may have reduced physiological reserve, making them more susceptible to the adverse effects of increased pulmonary pressures and resulting RV dysfunction if PE were to occur intraoperatively.5,7 Patients with a patent foramen ovale are also at increased risk during the PBSS procedure, as this condition can allow emboli to pass from the right to left side of the heart, potentially leading to stroke.
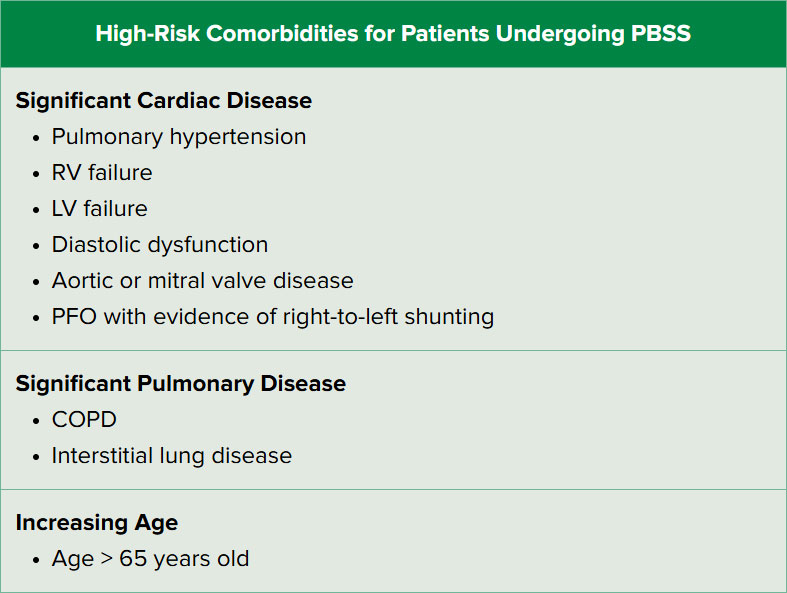
Figure 2. Identifying high-risk patients with reduced tolerance to intraoperative embolic events during the PBSS procedure.
Managing patients for this procedure can be challenging. Preoperatively, patients with known patent foramen ovale may benefit from placement of a vena cava filter to reduce the risk of embolic stroke. Ultrasound imaging can be used to locate the major venous outflow proximal to the planned surgical site so that if an embolus is suspected or identified, the vein can be compressed to potentially reduce or slow the embolic load entering the heart and lungs.
Arterial and/or central venous catheters may be beneficial in select patients, and in particularly high-risk patients a TEE probe can be placed preemptively following induction to monitor cardiac (particularly RV) function. Surgeons should notify the anesthesia team before monomer infusion and maintain ongoing communication throughout balloon inflation. In the event of pulmonary embolism, TEE may be useful to guide clinical management effectively. In cases of severe PE and RV dysfunction unresponsive to supportive measures, a cardiothoracic surgeon and a perfusionist may be required for the initiation of ECMO.8,9
In summary, utilization of the PBSS technique has increased in recent years, particularly for patients with metastatic metaphyseal lesions. While generally safe and well-tolerated, we suspect that hemodynamic instability and cardiovascular collapse during PBSS are underreported. Anesthesia providers should be aware that embolism of debris can occur due to an increase in intramedullary pressure during balloon expansion.10 Effective management of patients undergoing the PBSS procedure hinges on thorough patient risk stratification, clear team communication, vigilant intraoperative monitoring, and swift resuscitative efforts.
Taizoon Dhoon is an Associate Professor of Anesthesiology at UC Irvine Health, Orange, CA, USA
George Mina is a Medical Student at the UC Irvine School of Medicine, Irvine, CA, USA
Ramin Rahimian is an Associate Professor of Anesthesiology at UC Irvine Health, Orange, CA, USA
Shermeen Vakharia is a Professor of Anesthesiology at UC Irvine Health, Orange, CA, USA
Govind Rajan is a Professor of Anesthesiology at UC Irvine Health, Orange, CA, USA
None of the authors have any conflicts of interest.
Verbal consent to publish this case report was obtained from the patient.
REFERENCES
- IlluminOss Photodynamic Bone Stabilization System: All Forearm Surgical Technique. IlluminOss Medical. Published 2019. Accessed August 29, 2024. https://illuminoss.com/uploads/nuggets/5eaa859f7ee3385fc186902b/2019-All-forearm-surgical-technique-.pdf
- Zoccali C, Attala D, Pugliese M, di Uccio AS, Baldi J. The IlluminOss photodynamic bone stabilization system for pathological osteolyses and fractures of the humerus: indications, advantages and limits in a series of 12 patients at 24 months of minimum follow-up. BMC Musculoskelet Disord. 2021;22(1):63. doi:10.1186/s12891-020-03927-6. PMID: 33430839; PMCID: PMC7798276.
- Arcelus JI, Kudrna JC, Caprini JA. Venous thromboembolism following major orthopedic surgery: what is the risk after discharge? Orthopedics. 2006;29:506-516.
- Gausepohl T, Pennig D, Heck S, Gick S, Vegt PA, Block JE. Effective Management of Bone Fractures with the Illuminoss Photodynamic Bone Stabilization System: Initial Clinical Experience from the European Union Registry. Orthop Rev (Pavia). 2017;9(1):6988. doi:10.4081/or.2017.6988.
- Sabharwal S, Boland PJ, Vaynrub M. Severe Hemodynamic Collapse During Humerus Stabilization with Photodynamic Implant: A Report of Two Cases. JBJS Case Connect. 2024;14(2):e23.00634. doi:10.2106/JBJS.CC.23.00634. PMID: 38635765; PMCID: PMC11034895.
- Hope WW, Demeter BL, Newcomb WL, et al. Postoperative pulmonary embolism: timing diagnosis, treatment, and outcomes. Am J Surg. 2007;194:814-819.
- Kindler CH, Evgenov OV, Crawford LC, et al. Anesthesia for orthopedic surgery. In: Gropper M, Cohen NH, Eriksson LI, et al. Miller’s Anesthesia. 9th ed. Philadelphia, PA: Elsevier; 2019.
- Davies MG, Hart JP. Current status of ECMO for massive pulmonary embolism. Front Cardiovasc Med. 2023;10:1298686. doi:10.3389/fcvm.2023.1298686. PMID: 38179509; PMCID: PMC10764581.
- Hockstein MA, Creel-Bulos C, Appelstein J, Jabaley CS, Stentz MJ. Institutional experience with venoarterial extracorporeal membrane oxygenation for massive pulmonary embolism: a retrospective case series. J Cardiothorac Vasc Anesth. 2021;35(9):2681-2685. doi:10.1053/j.jvca.2020.12.045. PMID: 33531193.
- Bone cement implantation syndrome. ATOTW. Accessed August 29, 2024. https://resources.wfsahq.org/atotw/bone-cement-implantation-syndrome
