
Disclaimer: Viewers of this material should review the information contained within it with appropriate medical and legal counsel and make their own determinations as to relevance to their particular practice setting and compliance with state and federal laws and regulations. The APSF has used its best efforts to provide accurate information. However, this material is provided only for informational purposes and does not constitute medical or legal advice. This response also should not be construed as representing APSF endorsement or policy (unless otherwise stated), making clinical recommendations, or substituting for the judgment of a physician and consultation with independent legal counsel.
One of the most concerning developments in the ongoing and devastating worldwide COVID-19 pandemic is the emergence of serious and even life-threatening thrombotic complications in younger patients who contract the disease. Some patients have developed novel coronavirus-induced inflammatory changes which, along with platelet activation, endothelial dysfunction, and stasis, have produced a state similar to disseminated intravascular coagulation (DIC), with increased D-Dimer and fibrin/fibrinogen degradation products.1,2 COVID-19-associated hypercoagulable states have caused serious morbidity and mortality not typically seen in younger patients. 3,4,5
The clinical recommendations and clinical practice indications concerning thrombotic events from COVID-19 are multi-factorial and still evolving.6. For example, a recent online article highlighted a rather complicated set of 18 separate recommendations from the American College of Chest Physicians. These published guidelines cover a wide array of clinical situations for moderately, acutely, and critically ill COVID-19 patients. Interestingly, recommendations to both initiate and terminate apixaban (and similar drugs) are made at various points of the decision algorithm. Additionally, the Journal of the American College of Cardiology addressed thrombotic disease in COVID-19 patients and mentioned apixaban as a potential anticoagulation therapy.7
DDI Disclaimer: Our position in this article is not to provide comment on the advisability, efficacy, or validity of published guidelines and opinions on the management of microembolism and venous thromboembolism in the COVID-19 patient. Rather, we hope to provide and discuss additional information on apixaban DDIs that may be relevant to clinicians who are evaluating the co-administration of apixaban with a pre-existing medication panel.
Apixaban Basics
Apixaban is a direct-acting oral anticoagulant (DOAC). It is a direct inhibitor of Factor Xa in the coagulation cascade and it was approved by the FDA in December 2012 to reduce embolic events. Factor Xa, the common endpoint of the intrinsic and extrinsic clotting cascades, cleaves prothrombin to generate thrombin, promoting coagulation; thus, inhibition of Factor Xa produces a halt to the coagulation cascade. Apixaban is specifically approved to reduce the risk of stroke and systemic emboli in patients with nonvalvular atrial fibrillation (NVAF), to treat DVT and PE as well as reduce the risk of recurrence, and as prophylaxis for the prevention of DVT after knee or hip-replacement surgery.
The drug sheet for apixaban is available at HERE.
Drug-Drug Interaction Basics
Apixaban is a substrate of both the cytochrome (CYP) P450 3A4 enzyme (as well as several other CYP450 enzymes that make only a minor contribution to metabolism) and the P-glycoprotein (P-gp) pump (package insert). The CYP450 enzyme system is a family of enzymes important for the Phase I oxidative metabolism of various xenobiotics and endogenous compounds, such as steroid molecules. The most commonly encountered member of this family is the CYP3A4 enzyme, which comprises 30% of hepatic CYP450 activity and 70% of enteric CYP450 activity. CYP3A4 is responsible for contributing to the metabolism of 50-70% of medications currently in use. Even in the absence of genetic polymorphisms, clinicians should be mindful that there is a naturally occurring 10 to 30-fold variation in the metabolic efficiency of CYP3A4, leading to significant differences in how rapidly medications are metabolized across the population.
The P-gp transport system is an efflux pump found in the blood-brain barrier, kidney, liver, and gut luminal endothelial cells. DDIs occur with orally administered drugs when intestinal P-gp activity is either inhibited (increased bioavailability and higher concentrations of drug leading to increased risk of adverse effects) or induced ( reduced bioavailability of drug and decreased therapeutic effect).8
In the intestines, CYP3A4 often works in tandem with P-glycoprotein to create a barrier to intestinal absorption of substances, notably resulting in reduced bioavailability of many CYP3A4-metabolized medications. For example, an early study reported that orally-administered felodipine (a dihydropyridine calcium channel blocker) has its bioavailability reduced by greater than 80% after first-pass metabolism/efflux within enterocytes.9
Pharmacokinetic DDIs
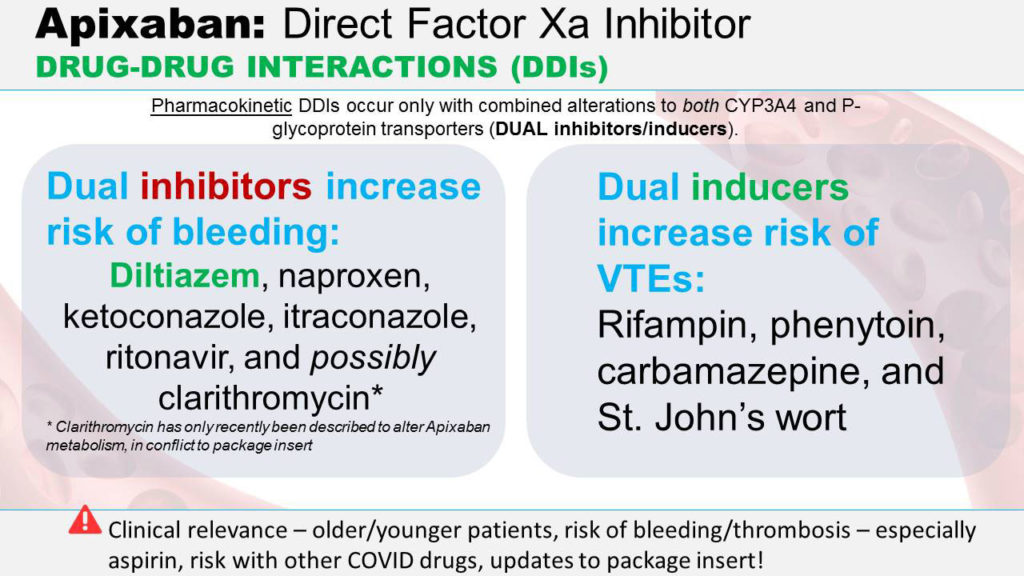
Apixaban is fairly unique in that only 25% of this drug is metabolized; the other 75% is ultimately excreted unchanged both via renal through urine and biliary excretion in feces. Therefore, in order for a change in pharmacokinetic handling of apixaban to produce any meaningful effects, there needs to be a synergistic alteration in BOTH metabolism via 3A4 AND absorption and distributional effects mediated by P-gp.
As a CYP3A4 substrate, apixaban is a participant in DDIs that involve both P-gp and 3A4 inhibitors and inducers.
The list of strong inhibitors of both 3A4 and P-gp that will meaningfully increase apixaban blood levels and anti-coagulation effects has been empirically demonstrated to include diltiazem, naproxen, ketoconazole, fluconazole, and ritonavir (package insert).10,11 Clinicians should be mindful that inhibition of CYP450 enzymes happens in a matter of several days or less (depending on the inhibitor). We also recommend that it would be especially worth the time for clinicians to review recent literature on the co-administration of apixaban and other DOACs with anti-viral medications, since lopinavir and/or ritonavir remain under active consideration for treatment of the novel coronavirus. For example, a recent Italian study investigated the trough blood levels of DOACs in COVID-19 patients who were admitted to the hospital on baseline DOAC therapy who received anti-viral therapies (lopinvir, ritonavir, or darunavir). Patients who had outpatient therapy DOAC stopped on admission were compared to patients who continued on outpatient dosages of DOAC while in the hospital. For the continuation patients, the investigators reported, “On average, C-trough levels were >6x higher during hospitalization than in the pre-hospital period.” The study authors attributed this “alarming” increase in DOAC levels to DDIs that have been reported to occur with coadministration of anti-viral agents and DOACs, including apixaban, but that clinicians failed to recognize.12,13
Interestingly, there is even emerging information that augments the package insert information. The package insert states, “Although clarithromycin is a combined P-gp and strong CYP3A4 inhibitor, pharmacokinetic data suggest that no dose adjustment is necessary with concomitant administration with ELIQUIS.” But a recent article, published June 11, 2020, describes a recent paper that seems to indicate that clarithromycin, when co-administered with apixaban and other direct oral anticoagulants, may confer hemorrhagic risk.
Conversely, only combined inducers of both CYP3A4 and P-gp will result in meaningful decreases in apixaban levels and increases in coagulability (package insert). These medications include rifampin, phenytoin, carbamazepine, and St. John’s wort. Induction of CYP450 enzymes happens over the course of several weeks as it involves an increase in the hepatic production of enzymes (which are proteins).
No inhibitory or induction effects on CYP3A4 (or the other CYP enzymes) or P-gp are seen with apixaban, so it is not expected to alter the metabolic clearance or absorption of co-administered drugs that are substrates of those systems.
Fortunately, apixaban has no effect on the QTc interval.
Pharmacodynamic DDIs
These interactions occur when two or more drugs have a synergistic or antagonistic effect at one receptor site or other site of action. There are straightforward pharmacodynamic DDIs that produce clinically meaningful interactions when DOACs (including apixaban) are co-administered with other anticoagulants. The packet insert mentions a higher rate of bleeding when apixaban is administered in patients receiving both single antiplatelet therapy with aspirin and dual antiplatelet therapy with aspirin and clopidogrel (APPRAISE-2 trial), as well as increased bleeding risk with concomitant use of aspirin and warfarin (ARISTOTLE trial).
Clinical Context
How might a review of DDIs pertaining to apixaban (and other DOACs) be helpful in maximizing patient safety for patients with the novel coronavirus?
First, younger patients appear to be at an elevated risk for both microembolism and other serious thromboembolic complications. Additionally, pre-hospital use of DOACs, including apixaban, is common in the older patient cohort that is at independent increased risk for COVID-19 illness. Therefore, clinicians may encounter apixaban in their patients’ medication panels.
Second, the clinical guidelines and recommendations for the use, initiation, and discontinuation of apixaban and other DOACs are still emerging and do not appear to be uniform at this time. It is generally a good practice for clinicians to be mindful of possible DDIs when medications are either stopped or started.
Third, the DDIs described above can result in vascular hemorrhage or decreased anticoagulant effect and embolic/thrombotic events. These clinical complications are potentially harmful for any patient but may be especially so for the medically complicated or fragile COVID-19 patient.
Fourth, there are recognized DDIs that involve apixaban and anti-viral medications, including lopinavir/ritonavir. These are all drugs that are currently under consideration for use in COVID-19 patients. Clinicians must be mindful of the unfortunate situation in which potential DDIs arise due to multiple indicated therapies.
Fifth, there is the unusual situation that emerging literature on apixaban DDIs supersedes the package insert. This involves a very recent report that found that clarithromycin may increase apixaban levels and risk of hemorrhagic events.
Conclusion
The possible DDIs arising from the use of apixaban and other DOACs demonstrate the complexity of caring for COVID-19 patients. Apixaban is not a primary therapy for the novel coronavirus, however clinicians may well encounter it in an existing medication panel and/or have the clinical indication to initiate or terminate this medication. Therefore, mindfulness and consideration of possible apixaban DDIs are always appropriate in order to maximize patient safety.
References
- Connors JM, Levy JH. COVID-19 and its implications for thrombosis and anticoagulation. Blood. Online ahead of print, 2020 Apr 27.
- Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up. J Am Coll Cardiol. 2020;S0735-1097(20)35008-7. Online ahead of print.
- Rennert RC, Wali AR, Steinberg JA, et al. Epidemiology, natural history, and clinical presentation of large vessel ischemic stroke. 2019;85(suppl_1):S4-S8.
- Thomas J Oxley, J Mocco, Shahram Majidi, et al. Large-vessel stroke as a presenting feature of Covid-19 in the young. N Engl J Med.2020;382(20):e60. Online ahead of print, 2020 Apr 28.
- Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Throm Res. 2020;191:145-147. Online ahead of print, 2020 Apr 10.
- Atallah B, Mallah SI, Al Mahmeed W. Anticoagulation in COVID-19. Eur Heart J Cardiovasc Pharmacother. Online ahead of print, 2020 Apr 30.
- Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and thrombotic and thromboembolic disease: implications for prevention, antithrombotic therapy, and follow up: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(23):2950-2973. Online ahead of print, 2020 Apr 17.
- Glaeser H. Importance of P-glycoprotein for drug-drug interactions. Handb Exp Pharmacol. 2011;(201):285-97.
- Edgar B, Regardh CG, Johnsson G, et al. Felodipine kinetics in healthy men. Clin Pharmacol Ther. 1985;3892:205-11.
- Nisly SA, Stevens BN. Ritonavir-or-cobicistate-boosted antiretroviral therapy and direct oral anticoagulants: a case for apixaban. Int J STD AIDS. 2019;30(7):718-722. Online ahead of print, 2019 Apr.
- Chang S-H, Chou I-J, Yeh Y-H. Association between use of non-Vitamin K oral anticoagulants with and without concurrent medications and risk of major bleeding in nonvalvular atrial fibrillation. JAMA 2017;318(13)1250-1259.
- Foerster KI, Hermann S, Mikus G, et al. Drug-drug interactions with direct oral anticoagulants. Clin Pharmacokinet. Online ahead of print, 2020.
- Gong IY, Kim RB. Importance of pharmacokinetic profile and variability as determinants of dose and response to dabigatran, rivaroxaban, and apixaban. Can J Cardiol. 2013;29(7 Suppl):S24‐ S33.
- Vazquez SR. Drug-drug interactions in an era of multiple anticoagulants: a focus on clinically relevant drug interactions. Hematology Am Soc Hematol Educ Program. 2018;339-347.
