Anesthetic management of patients with an anterior mediastinal mass (AMM) can be challenging, with its rarity adding complexity to the study of evidence-based management. This narrative review focusses on updates in anesthetic considerations for pediatric patients with AMM incorporating pertinent details for adult patients.
INTRODUCTION
Anesthetic management of an anterior mediastinal mass (AMM) is challenging, with its rarity adding complexity to the study of evidence-based management. The potential for airway and cardiovascular compromise and collapse leading to patient death are dreaded complications in the management of AMM. To prevent adverse outcomes, awake intubation, inhalational induction, spontaneous ventilation, and avoidance of neuromuscular blockade have been traditionally recommended. Recent studies evaluating airway and respiratory dynamics during general anesthesia in patients with AMM are changing the traditional management concepts. Other recent studies have provided new insights on risk stratification and preoperative planning for patients with AMM. Using available evidence, this narrative review provides updates in anesthetic considerations for management of pediatric patients with AMM incorporating pertinent details for adult patients.
RELEVANT ANATOMY
The pre-vascular (anterior) mediastinum, limited superiorly by the thoracic inlet, inferiorly by the diaphragm, anteriorly by the sternum, posteriorly by the pericardium, and laterally by the parietal mediastinal pleura, contains the thymus, lymph nodes, fat, and the left brachiocephalic vein. (Figures 1, 2 and 3)1,2. The visceral (middle) mediastinum contains trachea, esophagus, lymph nodes, heart, ascending thoracic aorta, aortic arch, descending thoracic aorta, superior vena cava, intrapericardial pulmonary arteries, and thoracic duct. The paravertebral (posterior) mediastinum contains soft tissue.
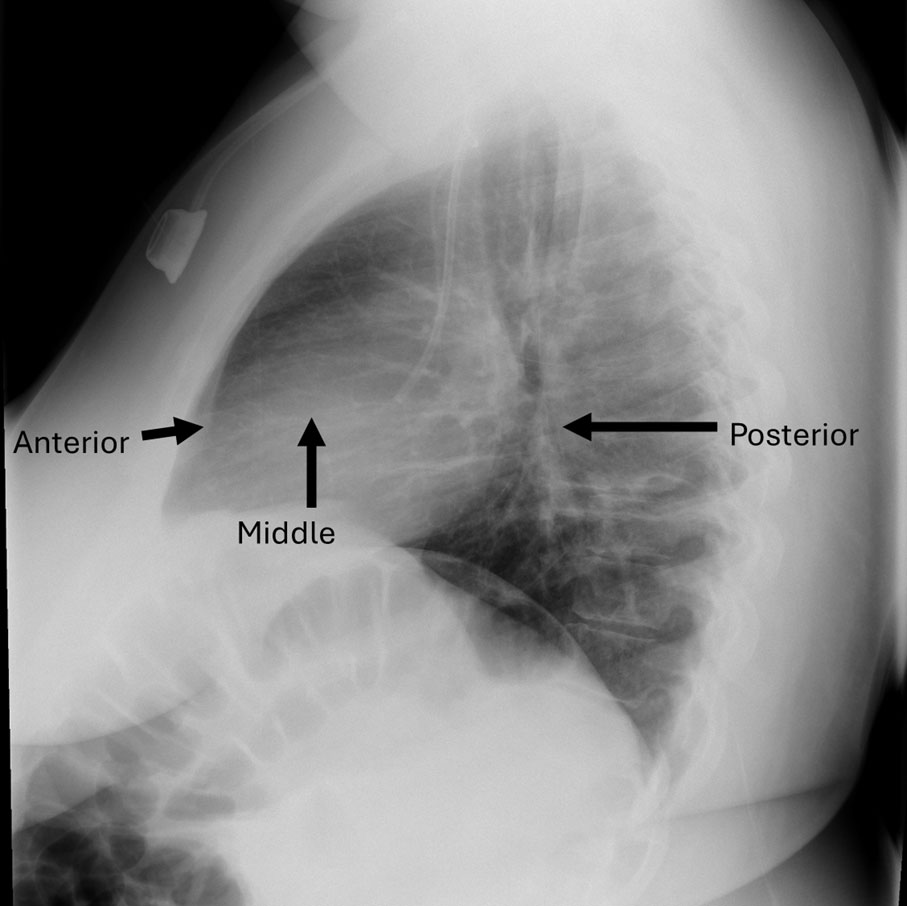
Figure 1. Lateral chest radiograph demonstrates anterior, middle and posterior mediastinal compartments.
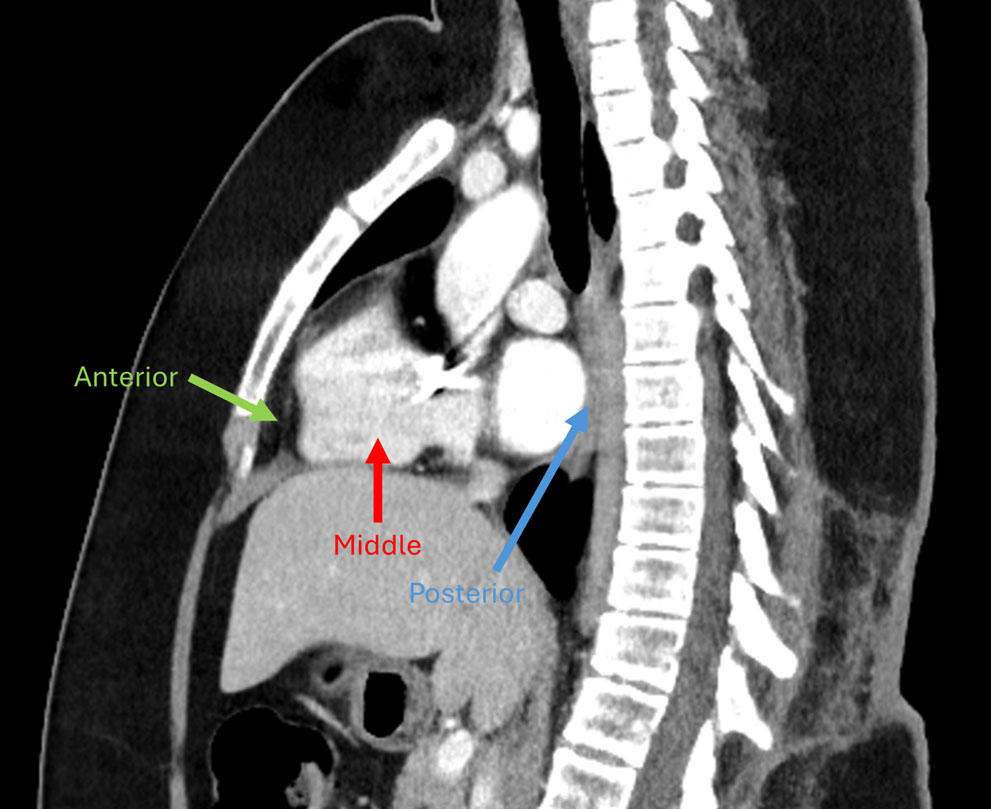
Figure 2. Computed tomography (CT) of chest, sagittal section demonstrates anterior, middle and posterior mediastinum.
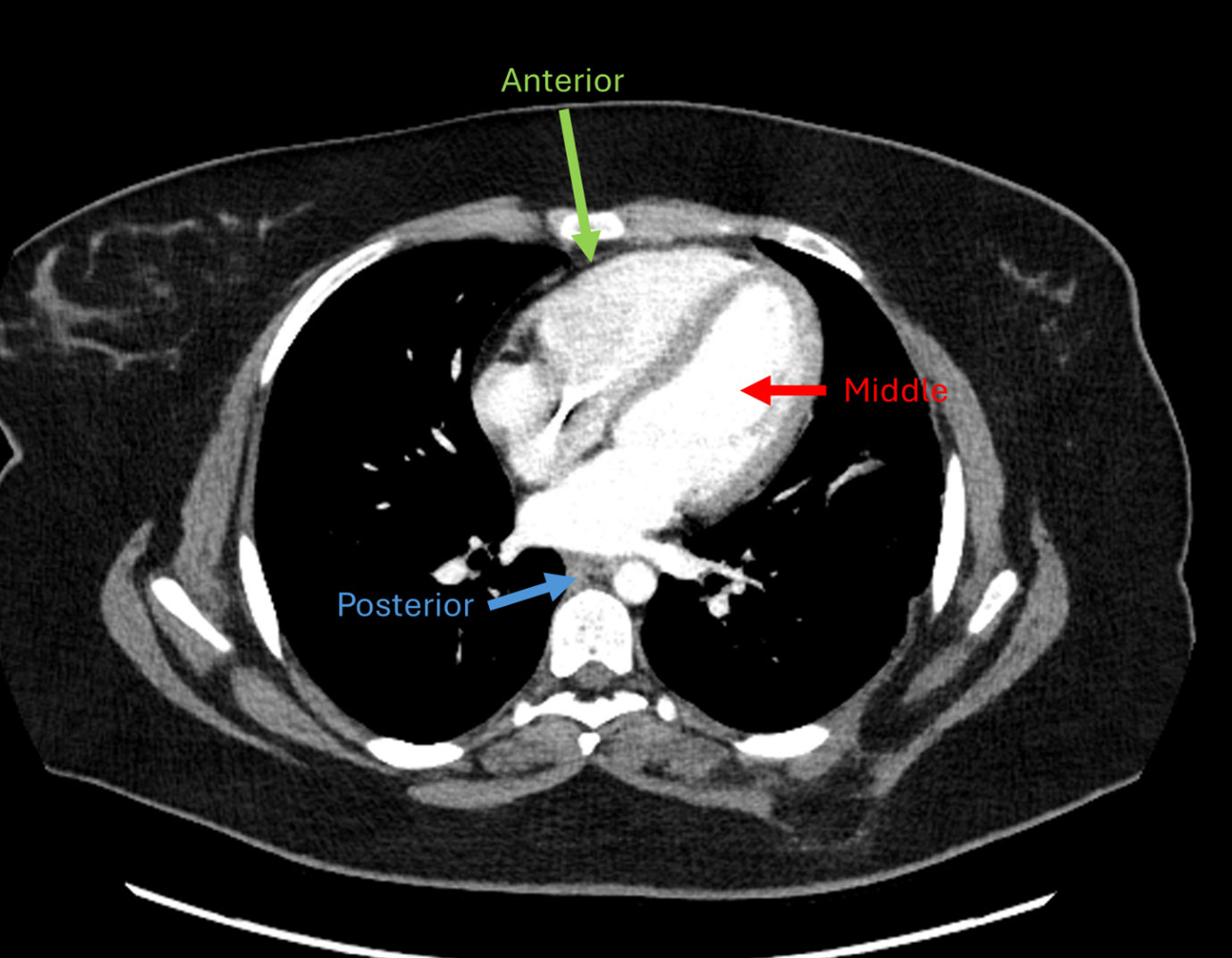
Figure 3. Computed Tomography (CT) chest, axial section demonstrates anterior (prevascular), middle (visceral), and posterior (paravertebral) mediastinum.
INCIDENCE AND TYPES OF MEDIASTINAL LESIONS
AMMs are metastatic lesions or originate from structures within or passing through mediastinum, representing about 3% of thoracic tumors. They have a bimodal distribution, with peak incidence occurring in children younger than ten years and adults aged sixty to seventy years.3 In adults, thymic lesions are the most common AMMs, followed by cysts and metastatic carcinomas. In children, lymphomas are the most common AMMs, followed by acute lymphoblastic leukemia and germ-cell tumors.
CLINICAL PRESENTATION
The clinical presentation of an AMM is determined by the rate of tumor growth and the degree of compression of adjacent structures. Symptoms include chest fullness, dyspnea, positional dyspnea including orthopnea, cough, stridor, hoarseness, dizziness, syncope, tachycardia, positional hypotension, and swelling of the face, neck, arms, and upper chest. Disease-specific symptoms may include fever, night sweats, and weight loss.
RELEVANT INVESTIGATIONS
After an initial chest X-ray (Figure 4), computed tomography (CT) angiography (Figures 5 and 6), transthoracic echocardiography, and pulmonary-function-tests guide presumptive diagnosis, treatment planning, and risk stratification (Table 1). In particular, spirometry helps with risk stratification in adult patients, by predicting post-operative respiratory complications, based on peak expiratory flow rate. Spirometry is unlikely to be meaningful in children due to limited cooperation and/or the urgency of presentation.
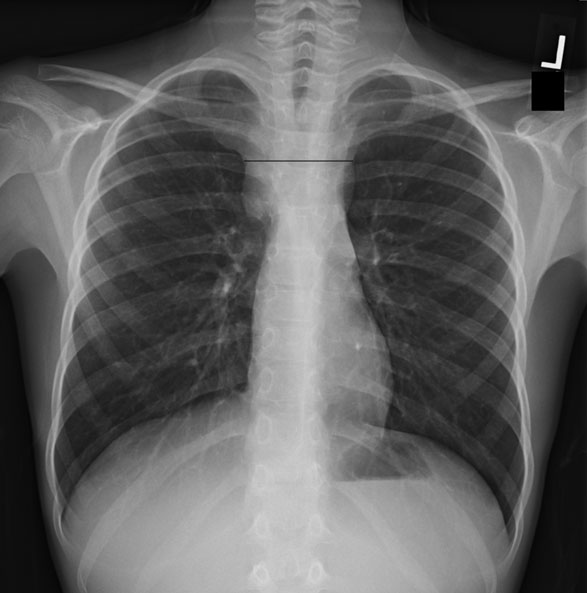
Figure 4. Chest radiograph demonstrates mediastinal widening due to anterior mediastinal mass.
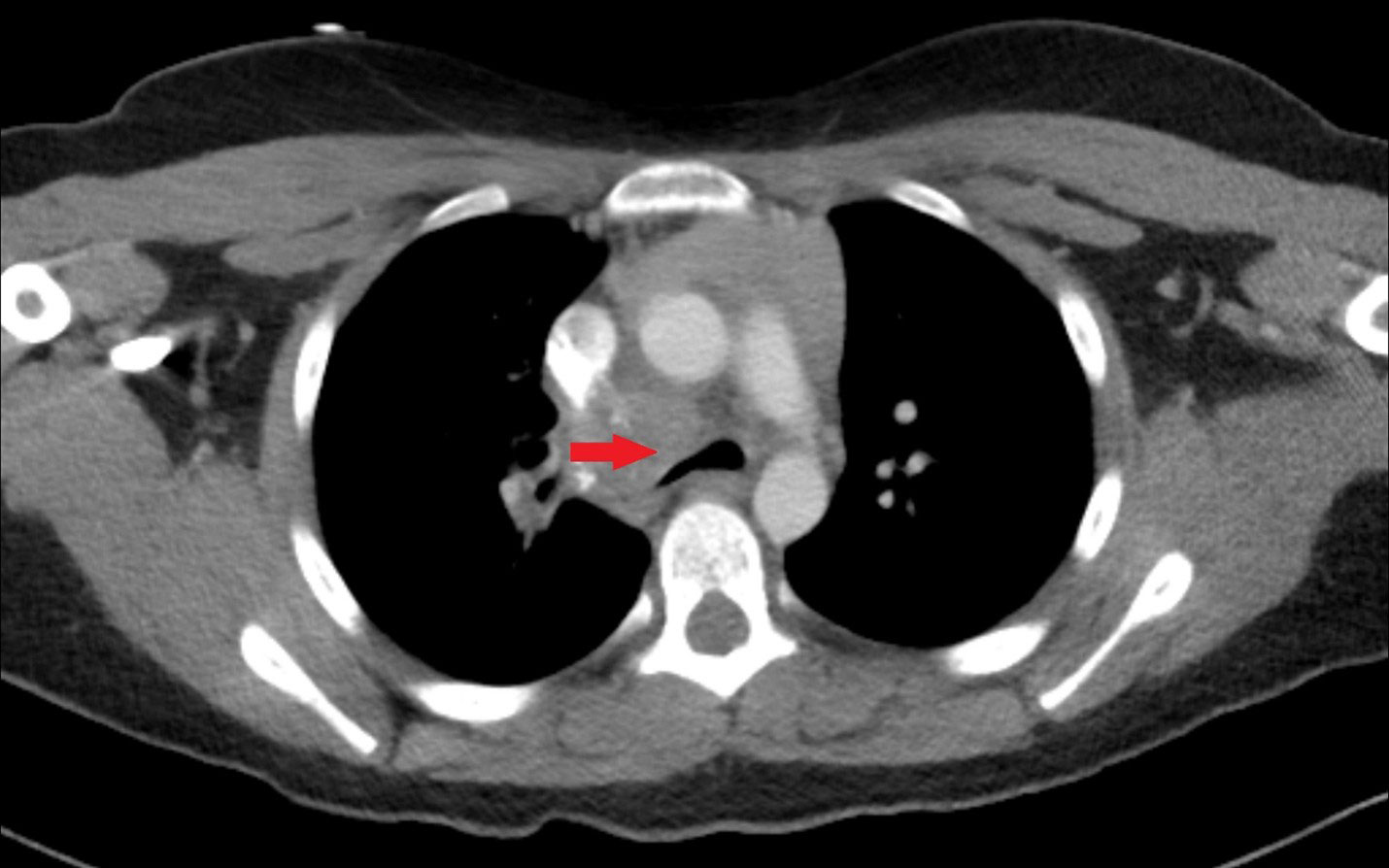
Figure 5. Chest CT of a 13-year-old demonstrates a right paratracheal soft tissue mass with associated tracheal compression.
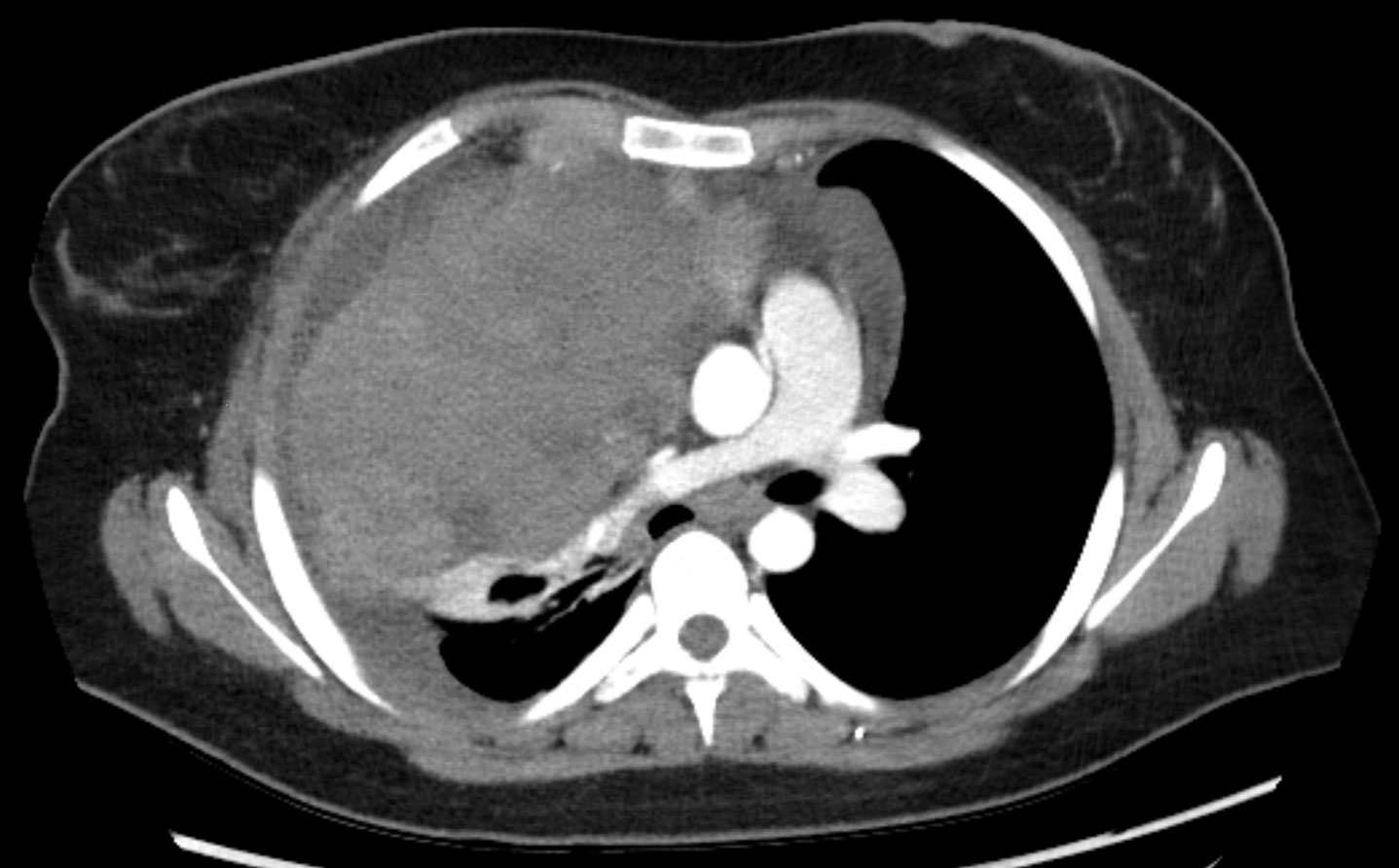
Figure 6. Chest CT of a 17-year-old with an anterior mediastinal mass with central airway and central vascular compression associated with the bulk disease, which raises concern for airway compromise.
Table 1. Diagnostic tests for anterior mediastinal mass evaluation.
| Diagnostic tests | Evaluation |
| Computed tomography (CT) angiography with thin slices and cardiac gating |
|
| Dynamic inspiration and expiration CT |
|
| Transthoracic echocardiography |
|
| Pulmonary function tests |
|
PATHOPHYSIOLOGY AND EFFECTS OF ANESTHESIA
In an upright healthy person, inspiration increases airway caliber, reducing the resistance to airflow. Expiration decreases airway caliber, increasing airway resistance. Supine positioning decreases functional residual capacity (FRC). Patients compensate for the compressive effects of an AMM by adopting a suitable body position and increasing inspiratory flow, expiratory flow, and expiratory time. These actions are compromised during anesthesia in the supine position because of diminished muscle tone and gravitational assistance that normally helps displace the mass away from the airway, even during spontaneous ventilation. Reduced lung volumes increase dynamic airway resistance and decrease pulmonary compliance. During positive pressure ventilation, airway caliber increases during inspiration but decreases during expiration. Air trapping can occur during expiration, leading to auto-positive end expiratory pressure (PEEP) if the expiratory time is not increased to account for decreased expiratory flow rate. Neuromuscular blockade worsens this situation by reducing respiratory muscle tone, leading to airway compression by the extraluminal AMM.
Awake patients with major vascular compression may be relatively asymptomatic. Compression of the superior vena cava leads to reduced venous return to the right atrium. Compression of the right ventricle or pulmonary artery compromises the right cardiac outflow. During anesthesia, loss of sympathetic tone, reduction in venous tone, relative hypovolemia, and increased intrathoracic pressure during positive pressure ventilation, especially in the event of air trapping, can compromise venous return and right-sided cardiac outflow. A pericardial effusion worsens these deleterious effects. After extubation, residual muscle weakness, increased work-of-breathing due to pain, sympathetic stimulation, and post–tumor resection tracheo-bronchomalacia can lead to cardiorespiratory compromise.
RISK STRATIFICATION
Patients with AMM can be risk stratified based on clinical signs and symptoms, tumor location, and diagnostic studies (Tables 2 and 3).4,5,1 Perioperative risk increases with symptom severity, progression, and positional nature of the AMM. Stridor, positional dyspnea, cyanosis, and signs of superior vena cava syndrome (upper body edema, indicating a severe degree of airway and vascular compression) are associated with higher risk of complications.6 Tracheal compression of >50% is associated with higher risk in children than in adults who have firmer cartilage and larger-diameter airways.6-11 In adults, a higher mass to chest ratio is associated with post-extubation airway complications.12 Pericardial effusion and superior vena cava obstruction are associated with a higher risk of hemodynamic compromise.6 The risk of respiratory complications is higher in adult patients with peak expiratory flow rate < 40% and with mixed obstructive restrictive patterns secondary to mediastinal mass.6
Table 2. Adult mediastinal mass perioperative risk stratification. (Adapted from Saffarzadeh et al, Annals of Thoracic Surgery. 2024.) a Superior Vena Cava b Pulmonary artery c Pulmonary function tests d Ventilation perfusion.
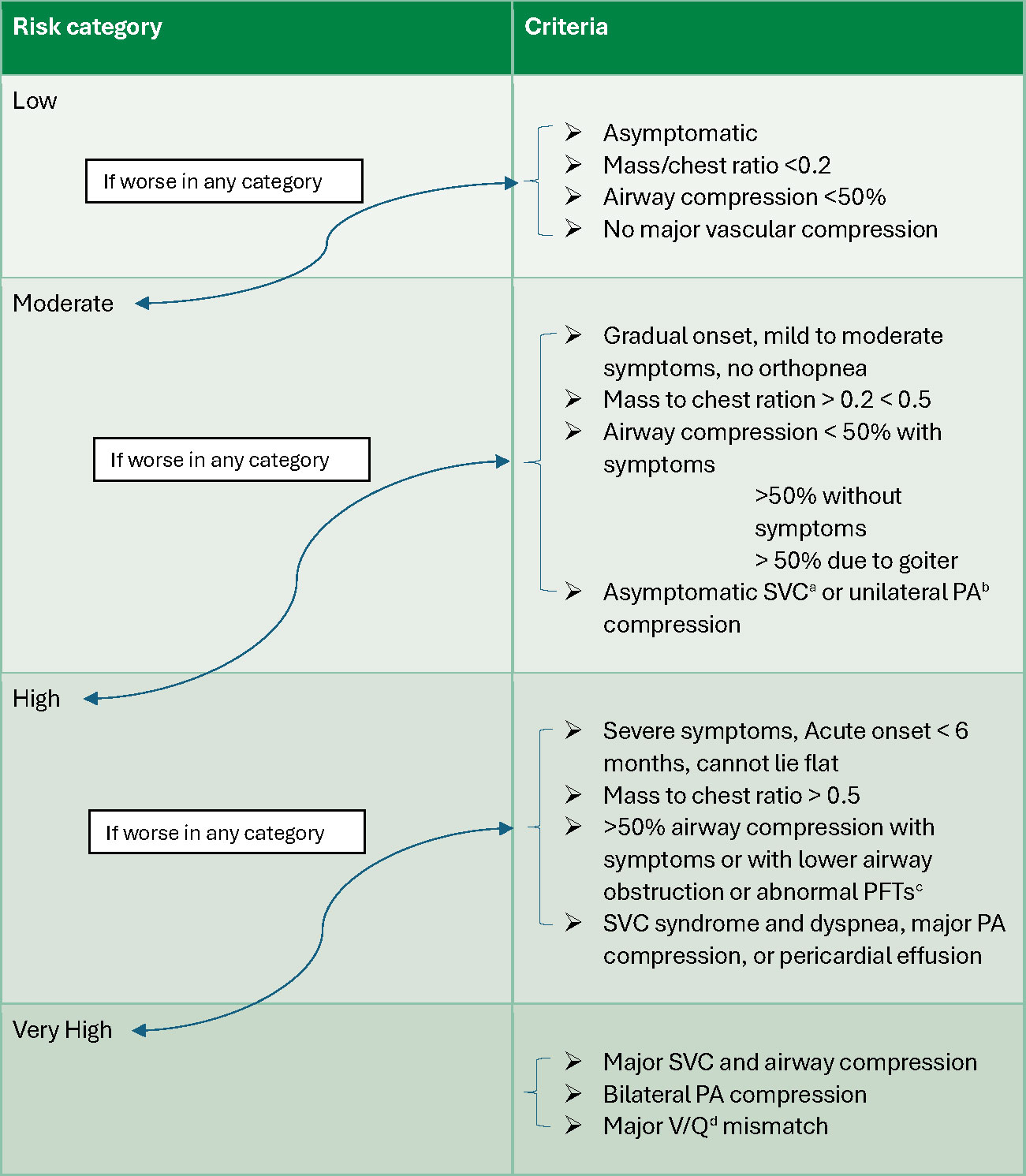
Table. 3. Pediatric mediastinal mass perioperative risk stratification (Adapted from Pearson et al, Seminars Cardiothoracic and Vascular Anesthesia 2015).
| Risk category | Criteria |
| Low |
|
| Moderate |
|
| Severe |
|
Though asymptomatic children can have complications, the presence of three or more symptoms, including evidence of tracheal or vascular compression, reduction in tracheal cross-section by > 70%, mild combined tracheal and bronchial compression, and an average mediastinal mass ratio (maximum diameter of the mass: maximum intrathoracic diameter) of 0.56 have been associated with a higher risk of respiratory and cardiovascular compromise.13-15 Standardized tumor volume (STV) which estimates tumor volume while accounting for a patient’s height, has more recently been identified as an imaging parameter for predicting the risk of respiratory collapse with general anesthesia in children with AMM.16
STV= 4/3 p (½ tumor height x ½ tumor width x ½ tumor depth)/ body height
ANESTHETIC CONSIDERATIONS
Multidisciplinary teams involving oncologists, radiologists, surgeons, otolaryngologists, and anesthesia professionals should proactively discuss the clinical presentation, risk categorization, procedural needs, and perioperative risks in patients with an AMM undergoing diagnostic and therapeutic procedures. Tumor, lymph node, or bone marrow biopsy are often required to establish a diagnosis. In children, central venous catheter placements for initiation of therapy may be required. Less invasive procedures, such as peripherally inserted central venous catheter and lymph node biopsies from superficial locations, should be also considered whenever possible. The anesthetic technique should be customized to the patient’s age, ability to tolerate anxiolysis or sedation, risk category, clinical condition, and planned procedure. The operating room is the preferred setting for initial procedures to ensure immediate availability of necessary resources such as experienced staff, wider selection of advanced airway devices and vascular access equipment and medications, allowing rapid escalation of care if needed.
Anxiolysis or mild to moderate sedation with locoregional anesthesia should be used in cooperative children and adults for less invasive procedures not requiring general anesthesia. Although there is no single preferred anesthetic agent, anxiolysis with intravenous midazolam or sedation with ketamine, dexmedetomidine, and remifentanil in combination with low-dose propofol, are commonly used. Preservation of airway reflexes with ketamine and dexmedetomidine, and rapid titratability of remifentanil render these drugs desirable for sedation in these patients. Routine techniques may be considered for asymptomatic patients at low risk having invasive procedures that require general anesthesia.
In moderate to high-risk patients, the goal should be to maintain spontaneous ventilation and an awake state. General anesthesia should be avoided, with the aim of avoiding cardiorespiratory complications. For patients at moderate or high-risk requiring general anesthesia, a discussion with oncologists about administering pre-diagnosis steroids to facilitate tumor size reduction and postponing the procedures to facilitate tumor burden reduction should be considered.14 The patient’s risk profile should be discussed in a multidisciplinary meeting well in advance of the general anesthesia in order to confirm the presence of heliox, jet ventilation, rigid bronchoscopy, airway stenting, and extracorporeal membrane oxygenation (ECMO) canulation resources to ensure their availability when needed, and clarify anticipated response times. If the patient is at high risk for airway or vascular collapse, transfer to a center with ECMO capabilities should be strongly considered. Adequate intravenous access in a lower extremity in the case of superior vena cava obstruction and possibly an arterial catheter, should be obtained prior to induction. After adequate preoxygenation, anesthesia should be induced slowly in a semi-sitting or other comfortable position resulting in the least patient dyspnea, while maintaining spontaneous ventilation. Muscle relaxants should be avoided. If an endotracheal tube is needed, the level of airway compression in relation to the tracheal tube should be reviewed preoperatively and an armored tracheal tube may be indicated. Although awake tracheal tube placement is ideal, it can be challenging in pediatric patients. A patient at moderate risk of airway collapse can be cautiously intubated while anesthetized and spontaneously breathing. Those at high risk should be intubated while awake or mildly sedated after adequate airway topicalization with local anesthetic. Short-acting drugs should be administered to deepen the anesthetic and determination of whether the patient will tolerate positive pressure ventilation should be assessed prior to administering muscle relaxants, which are ideally avoided. The traditional recommendation is to avoid positive pressure ventilation due to risk of cardiovascular collapse secondary to air trapping. Low respiratory rate with longer expiratory time to avoid air trapping should be used during positive pressure ventilation to avoid the same (Table 4). Performing fiberoptic bronchoscopy to visualize airway compression during patient positioning and prior to extubation helps guide rescue positioning and predict the need for post operative noninvasive ventilation, airway stenting, or external tracheal stabilization. Moderate to high-risk pediatric patients should be monitored in intensive care units postoperatively. Adult patients at moderate to high risk with post-extubation airway narrowing >50%, main stem bronchial compression, tracheomalacia, or abnormal spirometry prior to anesthesia should be monitored in intensive care settings.
Table 4 . Emerging concepts in airway and ventilation in patients with central intrathoracic airway obstruction22. PIF:Peak inspiratory flow; PEF:Peak expiratory flow; NMB: Neuromuscular blockade; PPV: positive pressure ventilation.
| Traditional concepts | Emerging concepts | |
| Awake spontaneous ventilation |
|
|
| Spontaneous ventilation during anesthesia. |
|
|
| Positive pressure ventilation during anesthesia. |
|
|
| Positive pressure ventilation during anesthesia with NMB. |
|
|
| Causes of hemodynamic collapse |
|
|
COMPLICATIONS
Airway obstruction during anesthetic induction is more common in younger patients with rapidly growing tumors while complications during or after extubation are common in older adult patients with large slow-growing tumors. In the event of airway obstruction efforts should focus on relieving airway compression before hypoxic arrest. Patient repositioning, guided by preprocedural imaging and patient’s symptomatology may help alleviate obstruction.18 Oxygenation should be maximized, spontaneous ventilation maintained and supported with CPAP. If respiratory obstruction persists, airways should be physically stented with a tracheal tube, a rigid bronchoscope, or an airway stent. In the case of persistent airway obstruction distal to the tracheal tube, ECMO should be initiated promptly to prevent cardiovascular collapse. In a high-risk patient if ECMO is anticipated, the circuit should be primed and immediately available, and the patient should be prepared for ECMO canula placement prior to induction of anesthesia. Although using ECMO in patients with cancer has been questioned, peripheral veno-venous ECMO has been used in the setting of tracheal compression resulting in severe hypoxia.19,20
Hemodynamic instability after induction can occur due to reduced venous return from the AMM compressing superior vena cava, right ventricle, or pulmonary artery; air trapping; hypoxic pulmonary vasoconstriction; or cardiac tamponade. Immediate fluid resuscitation and repositioning to alleviate mechanical compression and restore perfusion and/or ventilation are the first steps in management. However, contingency plans to rapidly escalate to ECMO should be in place as discussed above. Peripheral veno-arterial ECMO has a role in patients with cardiopulmonary failure related to AMM but is not always effective depending on location and structures involved.21 Evaluating differential hypoxia caused by AMM compression on specific structures is crucial.19
CONCLUSION
Thorough pre-anesthesia evaluation, risk stratification, multidisciplinary collaboration, and meticulous planning are key to achieving optimal outcomes for patients with AMMs having anesthesia. The least-invasive procedures which do not require general anesthesia should be considered whenever possible. Anxiolysis or mild to moderate sedation with locoregional anesthesia and spontaneous ventilation should be used in cooperative children and adults. In instances where mechanical ventilation, rigid bronchoscopy, or ECMO are anticipated, steroids should be strongly considered and the procedure postponed allowing for tumor size reduction. In case where general anesthesia is necessary in moderate to high-risk patients, contingency plans to rapidly escalate to rigid bronchoscopy, airway stent placement, and ECMO should be in place. Adopting appropriate risk stratification systems, establishing institutional guidelines towards local care or transfer of care, and setting previously agreed guidelines across disciplines are critical for safer patient care.
Kavitha C Raghavan is an associate member at St Jude Children’s Research Hospital, Memphis, Tennessee, United States of America, and an associate professor at University of Tennessee Health Science Center, Memphis, Tennessee, United States of America.
Joanna Rosing Paquin is an associate professor at Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio, United States of America.
The authors report no conflicts of interest.
REFERENCES
- Pearson JK, Tan GM. Pediatric Anterior Mediastinal Mass: A Review Article. Semin Cardiothorac Vasc Anesth. 2015;19(3):248-54. doi:10.1177/1089253215578931
- Carter BW, Tomiyama N, Bhora FY, et al. A modern definition of mediastinal compartments. J Thorac Oncol. 2014;9(9 Suppl 2):S97-101. doi:10.1097/jto.0000000000000292
- Liu T, Al-Kzayer LFY, Xie X, et al. Mediastinal lesions across the age spectrum: a clinicopathological comparison between pediatric and adult patients. Oncotarget. 29 2017;8(35):59845-59853. doi:10.18632/oncotarget.17201
- Hachenberg T, Schilling T, Kretzschmar M. Perioperative management of patients with mediastinal mass syndrome. Curr Opin Anaesthesiol. 2025;38(1):58-64. doi:10.1097/aco.0000000000001453
- Saffarzadeh A, Popescu WM, Detterbeck FC, Li AX, Blasberg JD. Anesthetic Risk with Large Mediastinal Masses: A Management Framework Based on a Systematic Review. Ann Thorac Surg. 2024;S003-4975(24):776-8. doi:10.1016/j.athoracsur.2024.09.011
- Béchard P, Létourneau L, Lacasse Y, Côté D, Bussières JS. Perioperative cardiorespiratory complications in adults with mediastinal mass: incidence and risk factors. Anesthesiology. 2004;100(4):826-34; discussion 5A. doi:10.1097/00000542-200404000-00012
- Marshall ME, Trump DL. Acquired extrinsic pulmonic stenosis caused by mediastinal tumors. Cancer. 1982;49(7):1496-9. doi:10.1002/1097-0142(19820401)49:7<1496::aid-cncr2820490731>3.0.co;2-3
- Shamberger RC, Holzman RS, Griscom NT, Tarbell NJ, Weinstein HJ, Wohl ME. Prospective evaluation by computed tomography and pulmonary function tests of children with mediastinal masses. Surgery. 1995;118(3):468-71. doi:10.1016/s0039-6060(05)80360-5
- Shamberger RC, Holzman RS, Griscom NT, Tarbell NJ, Weinstein HJ. CT quantitation of tracheal cross-sectional area as a guide to the surgical and anesthetic management of children with anterior mediastinal masses. J Pediatr Surg. 1991;26(2):138-42. doi:10.1016/0022-3468(91)90894-y
- Azizkhan RG, Dudgeon DL, Buck JR, et al. Life-threatening airway obstruction as a complication to the management of mediastinal masses in children. J Pediatr Surg. 1985;20(6):816-22. doi:10.1016/s0022-3468(85)80049-x
- Azarow KS, Pearl RH, Zurcher R, Edwards FH, Cohen AJ. Primary mediastinal masses. A comparison of adult and pediatric populations. J Thorac Cardiovasc Surg. 1993;106(1):67-72.
- Piro AJ, Weiss DR, Hellman S. Mediastinal Hodgkin’s disease: a possible danger for intubation anesthesia. Intubation danger in Hodgkin’s disease. Int J Radiat Oncol Biol Phys. 1976;1(5-6):415-9. doi:10.1016/0360-3016(76)90006-7
- Anghelescu DL, Burgoyne LL, Liu T, et al. Clinical and diagnostic imaging findings predict anesthetic complications in children presenting with malignant mediastinal masses. Paediatr Anaesth. 2007;17(11):1090-8. doi:10.1111/j.1460-9592.2007.02279.x
- Hack HA, Wright NB, Wynn RF. The anaesthetic management of children with anterior mediastinal masses. Anaesthesia. 2008;63(8):837-46. doi:10.1111/j.1365-2044.2008.05515.x
- Ng A, Bennett J, Bromley P, Davies P, Morland B. Anaesthetic outcome and predictive risk factors in children with mediastinal tumours. Pediatr Blood Cancer. 2007;48(2):160-4. doi:10.1002/pbc.20702
- Kawaguchi Y, Saito T, Mitsunaga T, et al. Prediction of respiratory collapse among pediatric patients with mediastinal tumors during induction of general anesthesia. J Pediatr Surg. 2018;53(7):1365-1368. doi:10.1016/j.jpedsurg.2017.09.013
- Feng J, Zhao J, Zhang Y, Hu Y. Incidence, outcome and risk factors of perioperative pulmonary complications in pediatric patients with mediastinal mass. BMC Pediatr. 12 2025;25(1):108. doi:10.1186/s12887-025-05419-9
- McLeod M, Dobbie M. Anterior mediastinal masses in children. BJA Educ. 2019;19(1):21-26. doi:10.1016/j.bjae.2018.10.001
- Leow L, Sampath HK, Yong KJ, et al. Rescue extracorporeal membrane oxygenation for massive anterior mediastinal masses. J Artif Organs. 2021;24(4):450-457. doi:10.1007/s10047-021-01264-6
- Bertini P, Marabotti A. The anesthetic management and the role of extracorporeal membrane oxygenation for giant mediastinal tumor surgery. Mediastinum. 2023;7:2. doi:10.21037/med-22-35
- Juan IC, Poorsattar SP, Banks DA, et al. The Anterior Mediastinal Mass-the Challenging Management of Hypoxemia Despite Peripheral Cannulation for ECMO. J Cardiothorac Vasc Anesth. 2021;35(10):3108-3117. doi:10.1053/j.jvca.2021.03.003
- Sarkiss M, Jimenez CA. The evolution of anesthesia management of patients with anterior mediastinal mass. Mediastinum. 2023;7:16. doi:10.21037/med-22-37
