 麻酔専門職は、患者安全の分野で一貫してリーダーとして活躍しており、麻酔作業スペースにおける手指衛生の重要性を長年認識してきた。1 手指の汚染は、麻酔作業スペース内の複数の保菌場所を介した病原菌の伝播と関連しており、医療者の手から培養された細菌と感染症を引き起こした病原菌のゲノム解析により、医療者が患者の感染症を引き起こす病原菌を伝播していることが確認されている。2,3,4 黄色ブドウ球菌(S. aureus)の麻酔作業スペースでの伝播は、手術部位感染(surgical site infection, SSI)リスク増加と関連している。5 実際、SSIのリスクは、病原菌が予防的抗菌薬に感受性のある場合で5倍以上、抗菌薬に耐性がある場合で9倍に増加する。6 このリスクを軽減させるために、SSIを予防する多面的なアプローチが示されている。7 手指衛生が多面的プログラムの一環として改善されると、黄色ブドウ球菌の伝播とSSIを大幅に減少させることができる。8,9 これらの結果は、麻酔専門職が先導して、すべての手術室スタッフによる手指衛生遵守の改善を促進するための推進力となるべきである。
麻酔専門職は、患者安全の分野で一貫してリーダーとして活躍しており、麻酔作業スペースにおける手指衛生の重要性を長年認識してきた。1 手指の汚染は、麻酔作業スペース内の複数の保菌場所を介した病原菌の伝播と関連しており、医療者の手から培養された細菌と感染症を引き起こした病原菌のゲノム解析により、医療者が患者の感染症を引き起こす病原菌を伝播していることが確認されている。2,3,4 黄色ブドウ球菌(S. aureus)の麻酔作業スペースでの伝播は、手術部位感染(surgical site infection, SSI)リスク増加と関連している。5 実際、SSIのリスクは、病原菌が予防的抗菌薬に感受性のある場合で5倍以上、抗菌薬に耐性がある場合で9倍に増加する。6 このリスクを軽減させるために、SSIを予防する多面的なアプローチが示されている。7 手指衛生が多面的プログラムの一環として改善されると、黄色ブドウ球菌の伝播とSSIを大幅に減少させることができる。8,9 これらの結果は、麻酔専門職が先導して、すべての手術室スタッフによる手指衛生遵守の改善を促進するための推進力となるべきである。
麻酔作業スペースは、患者、手術用ベッド、麻酔器、注入装置が取り付けられた点滴台、清潔な備品が入ったカート、カート内または別の薬剤ステーションに保管された薬剤などを含む複雑な環境である。麻酔専門職は、通常の麻酔業務中に患者や麻酔作業スペース内の複数の構成要素に触れる。10,11 このような複雑な環境では、病原菌の伝播を遮断し、感染の拡大を防ぐために、手指消毒が必要である。世界保健機関(World Health Organization, WHO)は、手指衛生を実施すべき場面を「手指衛生の5つのタイミング」と定義している。12 手指衛生が必要となるタイミングは次のとおりである。患者に触れる前、清潔/無菌操作の前、患者に触れた後、体液曝露リスクのある作業後、患者周辺の物品に触れた後(図 1)。12 WHOのおよび同様の推奨事項を遵守すると、麻酔専門職は、1時間あたり最低でも54回13、最大150回の手指衛生を実施する必要がある。11,13 しかし、ある研究によると、麻酔専門職は1時間に1回未満しか手指衛生を行っていない。14 明らかに、改善の余地は大きいと言える。環境のいたるところに病原体が存在していることを考えると、病原体の伝播を抑制するのが不可能に思えるかもしれない。しかし、ある研究では医療者の手指における黄色ブドウ球菌の数を100コロニー形成単位(colony-forming units, CFU)未満に減少させることは実現可能な目標であり、これにより患者を守る手助けができることが示唆されている。9,15
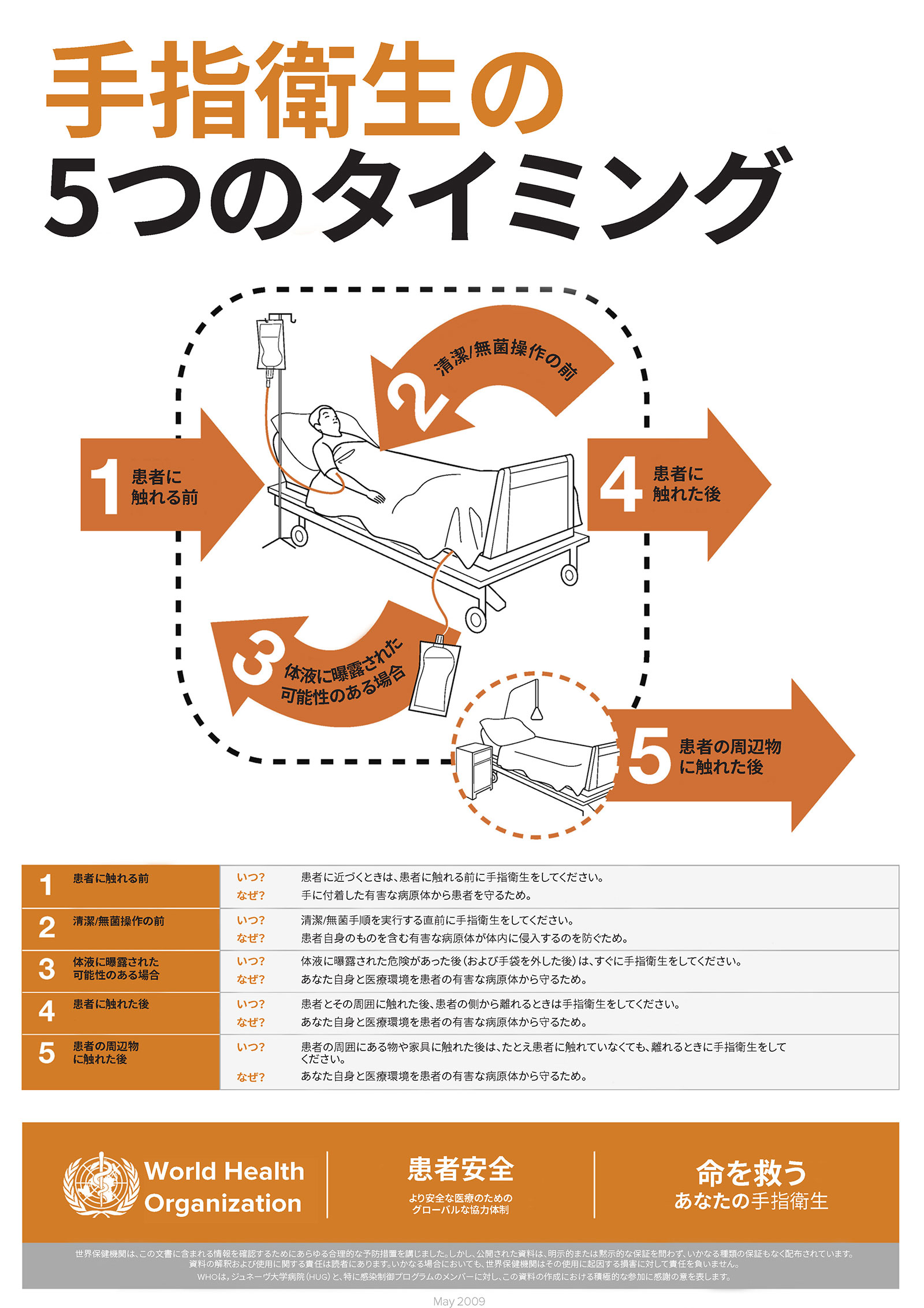
図1:手指衛生の 5 つのタイミングGeneva, Switzerland.World Health Organization.2009.ライセンス:CC BY-NC-SA 3.0 IGO.
APSF患者安全優先事項擁護グループの感染症班は、麻酔専門職が麻酔管理中の1時間に少なくとも約8回手指衛生を行うことを推奨している。16 1時間に8回の頻度で手を洗うか、手指消毒剤を使用することは、環境汚染や活栓汚染、そしてその後の感染症発生を最適に減少させた。14 しかし、この頻度で手指衛生の遵守を促すための適切な方法論は明確ではない。16 今後の重要な研究テーマとして、製品(例:アルコールベースのものまたは石鹸と水)、ディスペンサーの配置、洗浄技術、潜在的なリスクなどがある。
手指は、アルコールベースの消毒剤を使用すれば効果的に消毒できるが、目に見える汚染がある場合や芽胞形成細菌と接触した可能性がある場合は、石鹸と水で洗う必要がある。14,17 手洗い場は手術室の外に設置する必要があるため、麻酔専門職にとってはアルコールが主な手指衛生の選択肢となるが、これは石鹸と水よりも皮膚への刺激が少ないため、皮膚が炎症を起こしたり、炎症を起こした皮膚で細菌数が増加するリスクを軽減させたりする可能性がある。18,19
ディスペンサーの配置は、タスク密度(一定時間内に行う必要のあるタスクの数)によって決定するべきである。医療感染予防組織は、患者ケア領域内のアクセスしやすい場所にディスペンサーを配置することを推奨している。20 ディスペンサーを麻酔作業スペースの外(例えば、壁や手術室の入り口付近など)に設置すると、患者ケアが中断される可能性がある。タスク密度の重要性は明確に示されている。ある研究では、麻酔専門職が個人用の身体装着型アルコールディスペンサーを使用することで、手指衛生の遵守率が37倍増加し、その結果、環境汚染や活栓汚染、医療関連感染症の発生率が減少したと報告している。14 他の研究では、多面的プログラムの一環として、医療者の左側の点滴台にディスペンサーを設置した効果を評価した。8,9 この場所にディスペンサーを設置したことは、細菌伝播率とその後のSSI発症率を減少させた。8,9
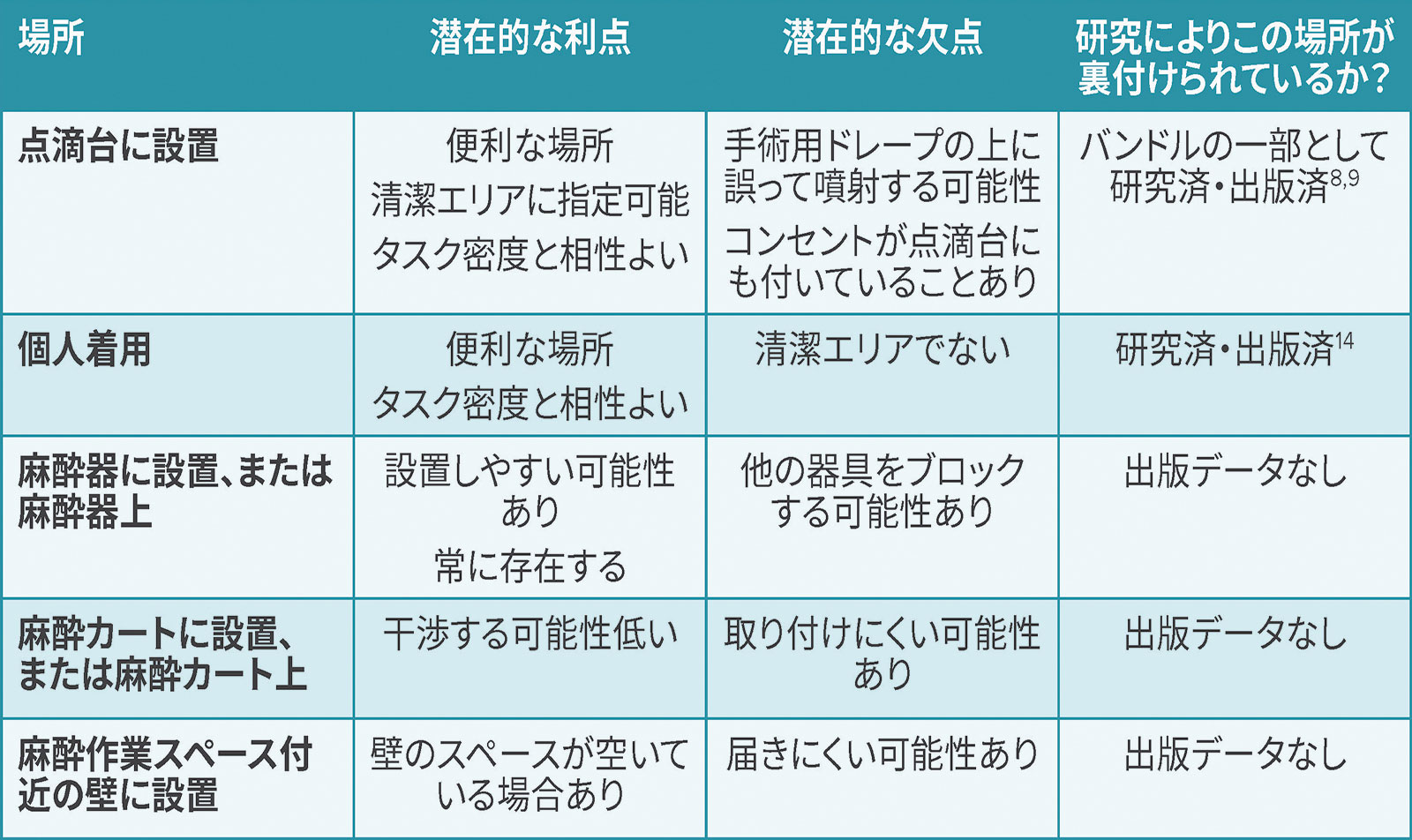
医療者の手指の汚染は環境汚染と関連しているため、環境清掃の頻度と質の向上も手指衛生の改善に役立つ可能性がある。ある研究では、麻酔作業スペースを「清潔」エリアと「汚染」エリアに分けると、100 CFU以上に達する部位の割合が減少することが判明した。14,21 アルコールディスペンサーは「清潔」エリアのほうに設置する必要がある。ディスペンサーは、取り付けラックを備えた麻酔器または麻酔カート、または点滴台に設置してもよい。点滴台に固定する場合は、患者、術野、電気プラグへの飛沫や滴下が起きないよう注意する必要がある(表 1)。
表 1:麻酔作業スペースにおける手指消毒剤の設置場所に関する潜在的な考慮事項
麻酔専門職は手指消毒剤に簡単にアクセスできる必要があるが、考慮すべき潜在的な危険性もある。すべてのアルコールベースの消毒剤には、60~80%のエタノールまたはイソプロピルアルコールと水が含まれている。水分が十分にあることが,微生物の膜を加水分解し、製品の蒸発を遅らせるために必要である。22,23 アルコール製品は可燃性であるため、消防法によって、室内に許可される消毒剤の総容量と、ディスペンサー間の最小距離が規制されている。ディスペンサーは最低でも4フィート(訳注:約1.2メートル)離して設置する必要があり、1つの部屋内のディスペンサーの合計容積は1.2リットルを超えてはならない。24 Centers for Disease Control(CDC)もこれらの火災安全に関する推奨事項を支持している。25 個人用に身体に装着するアルコールディスペンサーや点滴台に設置する片手用アルコールポンプの容量は3オンス(訳注:約90ミリリットル)未満である。8,9,14 手指消毒剤に関連した火災の報告はないが、リスクとしては考慮に値する。
要約すると、麻酔専門職による手指衛生の改善は、細菌伝播と感染症の発症を減少させるための多面的なアプローチにおいて不可欠な要素である。日常の麻酔管理中は、1時間あたり8回の手指衛生を行うことが奨励されている。麻酔作業スペース内のアルコールベースの消毒剤は、清潔でアクセスしやすい場所に設置し、医療者が明確に視認できるようにすべきである。
Jonathan E. Charnin, MD, FASAは、Mayo Clinic(ミネソタ州ロチェスター)の麻酔科および周術期医学部門の助教である。
Brendan T. Wanta, MDは、Mayo Clinic(ミネソタ州ロチェスター)の麻酔科および周術期医学部門の助教である。
Richard A. Beers, MDは、SUNYアップステート医科大学(ニューヨーク州シラキュース)の名誉教授ある。
Jonathan M. Tan, MD, MPH, MBI, FASAは、臨床麻酔科および空間科学の助教であり、ロサンゼルス小児病院および南カリフォルニア大学の集中治療医学部門、分析医療効果の副科長である。
Michelle Beam, DO, MBA, FASA, FACHEは、ペンシルバニア大学(ペンシルベニア州ウエストチェスター)医学部の麻酔科医である。
Sara McMannus, RN, BSN, MBAは、Sepsis Allianceの臨床アドバイザーである。
Desiree Chappel l , MSNA, CRNAは、NorthStar Anesthesia(テキサス州アービング)、臨床品質の副本部長である。
Randy W. Loftus, MDは、Mayo Clinic(ミネソタ州ロチェスター)の麻酔科および周術期医学部門の助教である。
Jonathan Tanは、APSF、Foundation for Anesthesia Education and Research (FAER)、Southern California Environmental Health Sciences Centerから研究助成金を受けており、GE HealthcareとEdwards LifeSciencesのコンサルタントである。
Desiree Chappellは、MedtronicとEdwards Life Sciencesの Speakers Bureau、ProVationの諮問委員会メンバーである。
Randy Loftusは、NIHによる研究資金(R01 AI155752-01A1)「BASIC試験: 細菌の伝播と感染を防ぐための証拠に基づくアプローチと監視の実施の改善」を報告している。APSF、Sage Medical Inc.、BBraun、Dräger、Surfacide、Kenallから資金提供を受けており、1つ以上の特許を申請中である。OR PathTracを所有するRDB Bioinformatics、LLCのパートナーであり、KenallとBBraunが主催する教育ミーテングで講演を行った。
他の著者には利益相反はない。
参考文献
- Warner MA, Warner ME. The evolution of the anesthesia patient safety movement in America: lessons learned and considerations to promote further improvement in patient safety. Anesthesiology. 2021;135:963–974. PMID: 34666350
- Dexter F, Loftus RW. Estimation of the contribution to intraoperative pathogen transmission from bacterial contamination of patient nose, patient groin and axilla, anesthesia practitioners’ hands, anesthesia machine, and intravenous lumen. J Clin Anesth. 2024;92:111303. Epub 2023 Oct 22. PMID: 37875062.
- Loftus RW, Brindeiro CT, Loftus CP, et al. Characterizing the molecular epidemiology of anaesthesia work area transmission of Staphylococcus aureus sequence type 5. J Hosp Infect. 2024;143:186–194. Epub 2023 Jul 13. PMID: 37451409.
- Loftus RW, Brown JR, Koff MD, et al. Multiple reservoirs contribute to intraoperative bacterial transmission. Anesth Analg. 2012;114:1236–1248. Epub 2012 Mar 30. PMID: 22467892.
- Hopf, Harriet W. MD. Bacterial reservoirs in the operating room. Anesthesia & Analgesia. 2015;120:p 700–702. PMID: 25790198
- Loftus RW, Dexter F, Brown JR. Transmission of Staphylococcus aureus in the anaesthesia work area has greater risk of association with development of surgical site infection when resistant to the prophylactic antibiotic administered for surgery. J Hosp Infect. 2023;134:121–128. doi: 10.1016/j.jhin.2023.01.007. Epub 2023 Jan 21. PMID: 36693592.
- Dexter F, Brown JR, Wall RT, Loftus RW. The efficacy of multifaceted versus single anesthesia work area infection control measures and the importance of surgical site infection follow-up duration. J Clin Anesth. 2023;85:111043. Epub 2022 Dec 23. PMID: 36566648.
- Loftus RW, Dexter F, Goodheart MJ, et al. The effect of improving basic preventive measures in the perioperative arena on Staphylococcus aureus transmission and surgical site infections: a randomized clinical trial. JAMA Netw Open. 2020;3: e201934. PMID: 32219407
- Wall RT, Datta S, Dexter F, et al. Effectiveness and feasibility of an evidence-based intraoperative infection control program targeting improved basic measures: a post-implementation prospective case-cohort study. J Clin Anesth. 2022; 77:110632. Epub 2021 Dec 17. PMID: 34929497.
- Sharma A, Fernandez PG, Rowlands JP, et al. Perioperative infection transmission: the role of the anesthesia provider in infection control and healthcare-associated infections. Curr Anesthesiol Rep. 2020;10:233–241. Epub 2020 Jul 17. PMID: 32837343
- Rowlands J, Yeager MP, Beach M, et al. Video observation to map hand contact and bacterial transmission in operating rooms. Am J Infect Control. 2014;42:698–701. PMID: 24969122
- WHO guidelines on hand hygiene in health care: first global patient safety challenge clean care is safer care. Geneva: World Health Organization; 2009. 21, The WHO Multimodal Hand Hygiene Improvement Strategy. Available from: https://www.who.int/publications/i/item/9789241597906. Accessed July 5, 2024
- Biddle C, Shah J. Quantification of anesthesia providers’ hand hygiene in a busy metropolitan operating room: what would Semmelweis think? Am J Infect Control. 2012;40:756–759. Epub 2012 Feb 9. PMID: 22325482.
- Koff MD, Loftus RW, Burchman CC, et al. Reduction in intraoperative bacterial contamination of peripheral intravenous tubing through the use of a novel device. Anesthesiology. 2009;110:978–985. PMID: 19352154.
- Dexter F, Walker KM, Brindeiro CT, et al. A threshold of 100 or more colony-forming units on the anesthesia machine predicts bacterial pathogen detection: a retrospective laboratory-based analysis. Can J Anaesth. 2024;71:600–610. English. Epub 2024 Feb 27. PMID: 38413516.
- Charnin JE, Hollidge M, Bartz R, et al. A best practice for anesthesia work area infection control measures: what are you waiting for? APSF Newsletter. 2022;37:103-106. https://www.apsf.org/article/a-best-practice-for-anesthesia-
work-area-infection-control-measures-what-are-you-waiting-for/ Accessed August 9, 2024. - WHO guidelines on hand hygiene in health care: first global patient safety challenge clean care is safer care. Appendix 2. Guide to appropriate hand hygiene in connection with Clostridium difficile spread. https://www.ncbi.nlm.nih.gov/books/NBK144042/. Accessed May 29, 2024.
- Pedersen LK, Held E, Johansen JD, Agner T. Short-term effects of alcohol-based disinfectant and detergent on skin irritation. Contact Dermatitis. 2005;52:82–87. PMID: 15725285
- Larson EL, Hughes CA, Pyrek JD, et al. Changes in bacterial flora associated with skin damage on hands of health care personnel. Am J Infect Control. 1998;26:513–521. PMID: 9795681
- Glowicz JB, Landon E, Sickbert-Bennett EE, et al SHEA/IDSA/APIC practice recommendation: strategies to prevent healthcare-associated infections through hand hygiene: 2022 update. Infect Control Hosp Epidemiol. 2023;44:355–376. PMID: 36751708
- Clark C, Taenzer A, Charette K, Whitty M. Decreasing contamination of the anesthesia environment. Am J Infect Control. 2014 Nov;42(11):1223-5. Epub 2014 Oct 30. PMID: 25444268.
- Ali Y, Dolan MJ, Fendler EJ, Larson EL. Alcohols. In: Block SS, ed. Disinfection, sterilization, and preservation. Philadelphia: Lippincott Williams & Wilkins, 2001:229–254.
- Rutala WA, Weber DJ, and the Healthcare Infection Control Practices Advisory Committee. Guideline for disinfection and sterilization in healthcare facilities, 2008. https://stacks.cdc.gov/view/cdc/47378 Accessed August 9, 2024.
- National Fire Protection Association (NFPA). NFPA 101 Life Safety Code. 2018 edition. Quincy, MA: National Fire Protection Association; 2018. https://www.nfpa.org/codes-and-standards/all-codes-and-standards/list-of-codes-
and-standards/detail?code=101 Accessed August 9, 2024. - Centers for Disease Control and Prevention (CDC). Clinical safety: hand hygiene for healthcare workers – fire safety and Alcohol-Based Hand Sanitizer (ABHS). https://www.cdc.gov/clean-hands/hcp/clinical-safety/?CDC_AAref_Val=https://www.cdc.gov/handhygiene/firesafety/index.htm Accessed July 5, 2024.
